Quick Reference
Inotropes Guide
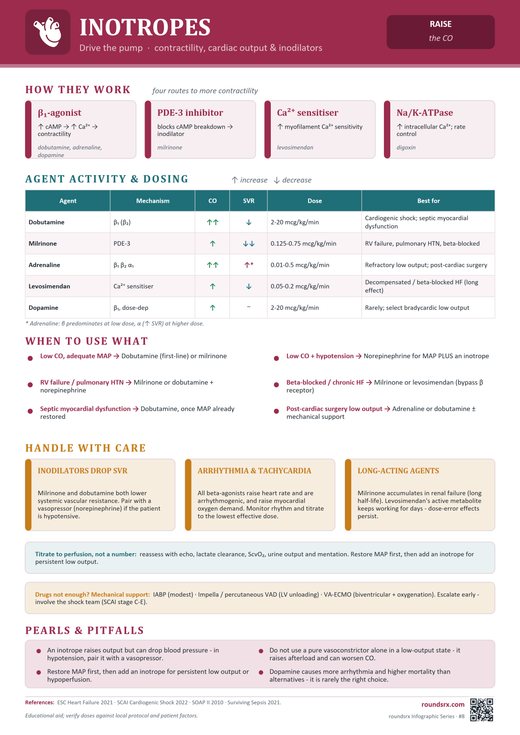
When the heart can't squeeze -agents that increase cardiac contractility. Know the hemodynamic profile of each before you hang the drip.
Inotropes ≠ vasopressors. Vasopressors increase SVR (squeeze vessels). Inotropes increase contractility (squeeze heart). Some agents do both. Picking the wrong one kills patients -a patient in cardiogenic shock who gets phenylephrine (pure vasoconstrictor, no inotropy) will get worse.
When to Use Inotropes
| Clinical Scenario | Hemodynamic Profile | Agent of Choice |
|---|---|---|
| Cardiogenic shock (acute MI, decompensated HFrEF) | ↓ CO, ↑ SVR, ↓ MAP, cold extremities, poor cap refill | Dobutamine (if BP adequate) or milrinone (if RV failure / pulm HTN). Add norepinephrine if MAP < 65. |
| Septic shock with cardiac dysfunction | ↓ CO despite adequate MAP on NE, poor ScvO₂ (< 70%), elevated lactate despite fluids + pressors | Dobutamine added to norepinephrine. Or epinephrine (provides both inotropy + vasopressor). SSC, 2021 |
| Acute RV failure (massive PE, pulm HTN crisis, RV infarct) | ↓ CO, ↑ CVP/JVP, ↑ PVR, RV dilation on echo, septal bowing | Milrinone (↓ PVR + inotropy) or dobutamine. Add inhaled epoprostenol/iNO for selective pulmonary vasodilation. Avoid volume loading -worsens RV dilation. |
| Post-cardiac surgery (low CO syndrome) | ↓ CO post-CPB, stunned myocardium | Milrinone (preferred -↓ afterload helps stunned heart, ↓ PVR). Or dobutamine. Epinephrine if hemodynamically significant. |
| Bridge to LVAD / transplant | End-stage HFrEF failing oral meds, awaiting mechanical support | Milrinone (continuous infusion, can use outpatient via PICC). Or dobutamine. |
| ADHF -"warm and wet" needing diuresis | Low CO limiting diuretic response, adequate BP | Low-dose dobutamine (2–5 mcg/kg/min) to augment renal perfusion for diuresis. Short-term only. |
Inotrope Comparison
| Agent (Brand) | Mechanism | Dose | Hemodynamic Effect | Best For | Watch Out |
|---|---|---|---|---|---|
| Dobutamine (Dobutrex) 1ST LINE |
β₁ > β₂ agonist | 2–20 mcg/kg/min IV | ↑ CO, ↑ HR, mild ↓ SVR (β₂ vasodilation). Net MAP may be unchanged or slightly ↓. | First-line inotrope in most cardiogenic shock (if MAP adequate). Septic shock with cardiac dysfunction. Augments diuresis in acute HF. | Never use alone if MAP < 65 -can drop BP via β₂ vasodilation. Always pair with NE if hypotensive. Tachycardia dose-limiting. Arrhythmogenic (↑ O₂ demand). Tachyphylaxis after 72h (downregulation of β-receptors). |
| Milrinone (Primacor) 1ST LINE |
PDE3 inhibitor (↑ cAMP) | 0.125–0.75 mcg/kg/min IV (skip loading dose in ICU -causes hypotension) |
↑ CO, ↓ SVR, ↓ PVR. "Inodilator" -inotropy + vasodilation. Better lusitropy (diastolic relaxation) than dobutamine. | RV failure / pulmonary HTN (↓ PVR is key advantage). Post-cardiac surgery. Bridge to LVAD/transplant. Works when β-receptors are downregulated (chronic HF on BB) -bypasses β-receptor. | Hypotension (vasodilation) -more than dobutamine. Renally cleared -dose-adjust in AKI/CKD. Thrombocytopenia (rare). Longer half-life (2–3h) -effects persist after stopping. Do NOT give loading dose in ICU (severe hypotension). |
| Epinephrine (Adrenalin) 2ND LINE |
α₁ + β₁ + β₂ agonist | Low dose: 0.01–0.1 mcg/kg/min (β₁/β₂ dominant → inotropy + vasodilation) High dose: 0.1–0.5 mcg/kg/min (α₁ dominant → vasoconstriction + inotropy) |
↑ CO, ↑ HR, dose-dependent SVR. Low dose = inotrope. High dose = inopressor. | Refractory cardiogenic shock (need both inotropy + pressor). Cardiac arrest. Post-arrest low CO. Anaphylaxis. | Falsely elevates lactate (β₂-mediated aerobic glycolysis) -cannot use lactate to guide resuscitation. Arrhythmogenic. ↑ myocardial O₂ demand. Hyperglycemia. Mesenteric ischemia at high doses. |
| Dopamine (Intropin) AVOID |
Dose-dependent: D₁ (low) → β₁ (mid) → α₁ (high) | "Renal dose" 1–3 → "cardiac" 3–10 → "pressor" 10–20 mcg/kg/min | Variable. Unpredictable hemodynamics. | Avoid. Inferior to NE in shock SOAP II, 2010. Only remaining role: symptomatic bradycardia if no pacing. | More arrhythmias and higher mortality vs NE. "Renal-dose dopamine" is a myth -no renal protection Bellomo, 2000. Unpredictable dose-response. Avoid in ICU. |
| Levosimendan (Simdax) SPECIALIZED |
Calcium sensitizer + K-ATP channel opener | 0.05–0.2 mcg/kg/min IV × 24h | ↑ CO, ↓ SVR, ↓ PVR. Inotropy without ↑ O₂ demand (unique). Active metabolite lasts 7–9 days. | Decompensated HF (Europe -not FDA-approved in US). Post-cardiac surgery. Bridge. Does not increase myocardial O₂ demand (unlike all other inotropes). | Not available in the US. Hypotension. Effect lasts days after stopping (long-acting metabolite). Limited data vs milrinone. |
| Isoproterenol (Isuprel) SPECIALIZED |
Pure β₁ + β₂ agonist (no α) | 2–20 mcg/min IV | ↑ HR, ↑ CO, ↓ SVR. Potent chronotrope. | Symptomatic bradycardia (bridge to pacing). Torsades de Pointes (↑ HR shortens QT). Beta-blocker overdose. Post-heart transplant (denervated heart -atropine doesn't work). | Severe hypotension (↓ SVR via β₂). Massively increases myocardial O₂ demand. Arrhythmogenic. Never use in ischemia. |
| Digoxin (Lanoxin) ADJUNCT |
Na⁺/K⁺-ATPase inhibitor → ↑ intracellular Ca²⁺ | 0.125–0.25 mg PO/IV daily Load: 0.25–0.5 mg IV |
Mild ↑ CO, ↓ HR (vagotonic). Weak inotrope compared to IV agents. | Chronic HFrEF with persistent symptoms on GDMT. Afib rate control adjunct (especially HFrEF). DIG, 1997: reduced HF hospitalizations, no mortality benefit. | Narrow therapeutic window (target 0.5–0.9 ng/mL). Toxicity: any arrhythmia -classically "regularized Afib" (junctional rhythm), bigeminy, bidirectional VT. Hypokalemia potentiates toxicity. Renally cleared -dose-adjust. Reversal: digoxin-specific Fab (DigiFab). |
Inotrope vs Vasopressor -Know the Difference
| Feature | Inotrope | Vasopressor | Inopressor (Both) |
|---|---|---|---|
| Primary effect | ↑ Contractility (↑ CO) | ↑ SVR (↑ MAP) | ↑ CO + ↑ SVR |
| Main receptor | β₁, PDE3 | α₁, V1 | α₁ + β₁ |
| Examples | Dobutamine, milrinone | Phenylephrine, vasopressin | Norepinephrine, epinephrine |
| Effect on SVR | ↓ or neutral | ↑↑ | ↑ |
| Use when | CO is low, MAP is OK | MAP is low, CO is OK | Both MAP and CO are low |
| Cardiogenic shock | Yes (primary) | Only as adjunct for MAP | NE is first-line pressor in CS |
| Septic shock | Add if ↓ CO despite MAP-targeted NE | NE is first-line | Epi if refractory |
Decision Flowchart
Is MAP < 65? → Start norepinephrine first (inopressor). You need MAP before you add a pure inotrope.
MAP adequate but CO is low? (cold extremities, poor cap refill, ↑ lactate, low ScvO₂) → Add dobutamine (first-line inotrope).
RV failure or pulmonary HTN? → Milrinone preferred (↓ PVR). Consider inhaled epoprostenol or iNO for selective pulmonary vasodilation.
Patient on chronic beta-blocker? → β-receptors are downregulated. Milrinone works better than dobutamine (PDE3 pathway bypasses β-receptor).
Need both inotropy + vasopressor? → Epinephrine (inopressor). Or NE + dobutamine as separate drips (more titratable).
Refractory to all above? → Mechanical circulatory support: IABP, Impella, ECMO. Call your interventional cardiology / cardiac surgery team early.
Key Pearls
All inotropes increase myocardial O₂ demand (except levosimendan). In ischemic cardiogenic shock, this is a double-edged sword -you're helping the pump but potentially worsening the ischemia. Keep doses as low as effective.
"Renal-dose dopamine" is a myth. Bellomo, 2000: no renal protection. SOAP II, 2010: more arrhythmias + higher mortality than NE. There is no role for dopamine as an inotrope in modern ICU care.
Dobutamine tachyphylaxis occurs after ~72h due to β₁-receptor downregulation. If the patient stops responding, switch to milrinone (PDE3 pathway) or add mechanical support.
Milrinone has a 2–3h half-life. If the patient drops their BP on milrinone, the effect persists for hours after stopping -unlike dobutamine (t½ ~2 min). Plan accordingly. Also: renally cleared -dose-reduce in AKI.
Epinephrine falsely elevates lactate via β₂-mediated aerobic glycolysis. If you're running epi for inotropy, you cannot use lactate clearance to assess resuscitation adequacy. Use ScvO₂, echo, or CI instead.
Digoxin toxicity = "any arrhythmia." Classic: regularized afib, bigeminy, bidirectional VT. Hypokalemia potentiates it. Always check K⁺ with dig level. Reversal: DigiFab (digoxin-specific Fab fragments).