The why behind
every decision.
Diabetic Ketoacidosis (DKA)
- Type 1 DM (can be the presenting illness in ~25%)
- Type 2 DM under physiologic stress
- SGLT2-inhibitor users (euglycemic DKA -BG may be < 200!)
- Precipitants: infection (30–40% -most common), insulin omission/non-compliance (20–25%), new diagnosis T1DM, MI/ACS, pancreatitis, cocaine, alcohol
Infection (30–40%, #1 cause -UTI, pneumonia, skin) · Insulin (missed or inadequate doses) · Infarction (MI, stroke, mesenteric ischemia) · Intoxication (cocaine, alcohol, drugs) · Inflammation (pancreatitis, surgery, trauma)
- Polyuria, polydipsia, nausea, vomiting, abdominal pain
- Weakness, fatigue, altered mental status (in severe cases)
- Timeline: hours to days (faster than HHS)
- Kussmaul respirations (deep, rapid -compensating for acidosis)
- Fruity/acetone breath
- Signs of dehydration: dry mucosa, tachycardia, hypotension, poor skin turgor
- Altered mental status → think cerebral edema, severe osmolarity
- Potassium < 3.5 → do NOT start insulin until repleted
- Euglycemic DKA (SGLT2i) -don't miss it
- pH < 7.0 or bicarb < 10 → severe DKA, ICU threshold
- HHS -BG often > 600, severe hypertonicity, no/minimal ketones, pH usually > 7.3
- Alcoholic ketoacidosis -low or normal glucose, ketones present, history of binge drinking + poor PO
- Starvation ketosis -mild, pH > 7.3, bicarb usually > 18
- Other high AG acidosis -lactic acidosis, toxic ingestions (methanol, ethylene glycol, salicylates)
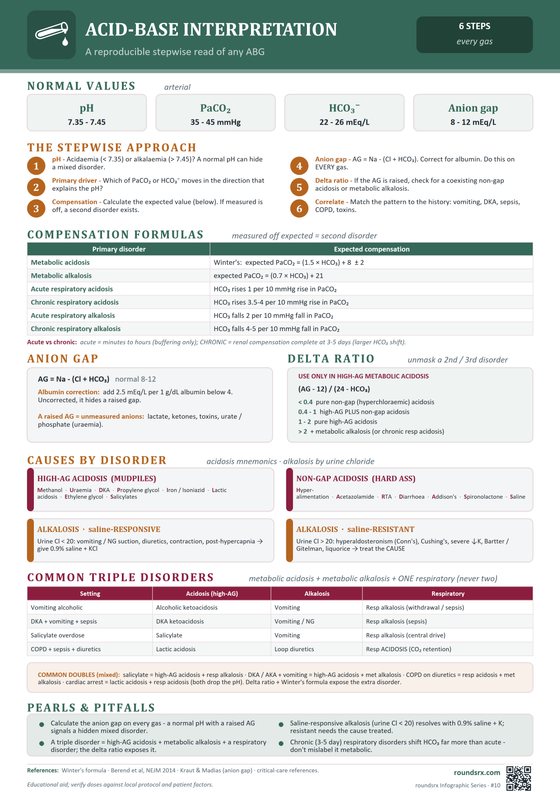
- BMP -BG, creatinine, K⁺, bicarbonate
- VBG or ABG -pH, pCO₂, calculated bicarb
- Anion gap = Na – (Cl + HCO₃) → normal 8–12; in DKA typically > 20
- Beta-hydroxybutyrate (BHB), serum -≥ 3.0 mmol/L is diagnostic for DKA per ADA/EASD 2024. Preferred over urine ketones for both diagnosis AND monitoring resolution.
- Urine ketones (only if serum BHB unavailable; moderate-to-large dipstick ketones is the fallback diagnostic threshold)
- Phosphate, magnesium -often depleted
- CBC, blood cultures -rule out infectious precipitant
- Lipase -DKA can elevate lipase without true pancreatitis
- HbA1c -assess chronic control
- Urinalysis + urine culture
- Pregnancy test (women of childbearing age)
- ECG -assess for hyperkalemia changes (peaked T waves, wide QRS) or ischemia as precipitant
- CXR -rule out pneumonia as precipitant
- CT head only if focal neuro deficits or concern for cerebral edema
- Hyperglycemia: glucose ≥ 200 mg/dL (or known diabetes; not required in euglycemic DKA on SGLT2i)
- Ketosis: BHB ≥ 3.0 mmol/L (preferred) OR moderate-to-large urine ketones
- Acidosis: venous pH < 7.3 OR serum bicarbonate < 18 mEq/L
| Parameter | Mild | Moderate | Severe | vs prior guideline |
|---|---|---|---|---|
| Venous pH | 7.25–7.30 | 7.00–7.24 | < 7.00 | UNCHANGED |
| Bicarb (mEq/L) | 15–18 | 10–<15 | < 10 | CHANGED mild now 15–18 (was 15–18, but resolution threshold raised) |
| Anion gap and mental status were removed from severity grading in 2024. AG is still elevated in DKA but is confounded by hyperchloremic acidosis after NS resuscitation. Altered mental status remains an independent ICU-triage criterion. | ||||
ABCs. IV access × 2. Foley if altered or unable to void. Cardiac monitor. POC glucose. Draw all STAT labs. Call senior if severe (pH < 7.1, AMS, K⁺ < 3.5).
• Unstable / severely volume-depleted: 1-1.5 L isotonic crystalloid bolus over 1 hour (NS OR balanced).
• Stable: skip the bolus -start 250-500 mL/hr maintenance from the outset.
The reflex "2 L for everyone" is out; over-resuscitation is the more common modern error ADA DKA Consensus, 2024
After the first hour, choose by corrected Na⁺ (calculator):
• Corrected Na ≤ 135 → continue 0.9% NS at 250-500 mL/hr
• Corrected Na > 135 → switch to 0.45% NaCl at 250-500 mL/hr
• If using LR: just continue LR throughout and skip the half-NS switch (LR's Na 130 already provides some free water; only switch to 0.45% NaCl if corrected Na > 150).
Goal: replace 3-6 L deficit over 24-48 h (gentler is fine; over-aggressive correction risks cerebral edema, especially in pediatrics -PECARN, 2018).
K⁺ < 3.5 → replace aggressively (20–40 mEq/hr IV), do NOT start insulin yet
K⁺ 3.5–5.0 → add 20–30 mEq K⁺ per liter of IVF, start insulin
K⁺ > 5.0 → start insulin, hold K⁺ replacement, recheck in 2 hours
Insulin Infusion
Regular insulin drip at 0.14 units/kg/hr (no-bolus protocol, per ADA 2026). Alternative: 0.1 unit/kg IV bolus + 0.1 unit/kg/hr infusion. Target: BG drop of 50–75 mg/dL/hr.
Add D5 to IV fluids (D5-0.45%NS) -reduce insulin drip to 0.05 units/kg/hr. Continue until anion gap closes, NOT just until BG normalizes. This is the most common resident mistake.
- Beta-hydroxybutyrate (BHB) < 0.6 mmol/L
- AND patient tolerating PO / clinically improved
- Venous pH ≥ 7.3
- Serum bicarbonate ≥ 18 mEq/L
- Anion gap ≤ 10 mEq/L
- pH < 7.0 or bicarb < 10
- Altered mental status / decreased GCS
- Hemodynamic instability not responding to fluids
- K⁺ < 3.0 or > 6.0 with ECG changes
- Concurrent MI, stroke, or surgical emergency
Patient: 28F with T1DM, glucose 520, pH 7.15, bicarb 8, AG 28, K⁺ 5.8
| Time | Action |
|---|---|
| Hour 0 | Start insulin drip 0.14 units/kg/hr (no bolus). NS 1L/hr. Do NOT give K⁺ yet (K⁺ > 5.2). |
| Hour 2 | Glucose 380 (↓140). K⁺ 4.5 → start KCl 20 mEq/hr in IV fluids. Continue insulin drip. |
| Hour 4 | Glucose 280 (↓100/hr -on target). K⁺ 3.8 → increase KCl to 40 mEq/hr. AG closing (18). |
| Hour 6 | Glucose 240 → approaching 250 threshold. Switch fluids to D5 1/2NS + KCl to prevent hypoglycemia while continuing insulin to close the gap. |
| Hour 8 | Glucose 190, pH 7.32, bicarb 16, AG 12 (closing). K⁺ 4.0. |
| Hour 10 | AG closed (AG 10), pH 7.38, bicarb 20, patient eating. → Overlap SC insulin (give long-acting + meal dose), wait 2 hours, THEN stop drip. |
Key: Never stop insulin drip until: (1) BHB < 0.6 mmol/L (or if BHB unavailable, AG ≤ 10), (2) pH ≥ 7.3, (3) bicarb ≥ 18, (4) patient eating, AND (5) SC insulin given ≥ 2h prior.
Patient: 52F with T2DM on empagliflozin + metformin. Presents with nausea, vomiting, abdominal pain × 2 days. Glucose 185 (not elevated!). pH 7.18, bicarb 10, AG 24, ketones 5.2.
The trap: Glucose is near-normal → team almost missed DKA. SGLT2 inhibitors cause glycosuria → glucose stays low while ketoacidosis develops.
Treatment:
- Stop empagliflozin immediately. Effects last 24–48h even after stopping.
- Start D5NS + insulin drip, need dextrose from the start since glucose is already normal. Cannot let glucose drop further.
- Aggressive K⁺ monitoring, same protocol as classic DKA.
- Close the gap: Same endpoints, pH > 7.3, bicarb > 18, AG closed. Takes longer than classic DKA because you're limited by how fast you can run insulin with dextrose.
Key lesson: Always check a VBG/BMP on any patient on SGLT2i presenting with nausea/vomiting. Normal glucose does NOT rule out DKA. Check ketones and AG.
Patient: 19M with T1DM, found unresponsive. Glucose 680, pH 6.95, bicarb 4, AG 36. K⁺ = 2.8.
Critical decision: K⁺ < 3.3 → DO NOT start insulin yet. Insulin drives K⁺ intracellular → can cause fatal arrhythmia.
Treatment:
- Step 1: IV KCl 40 mEq/hr via central line (peripheral max 10 mEq/hr). Continuous telemetry. Recheck K⁺ every 1–2 hours.
- Step 2: Aggressive IVF, NS 1L/hr. Fluids alone will lower glucose ~50–75 mg/dL/hr.
- Step 3: Once K⁺ ≥ 3.3 → START insulin drip at 0.14 units/kg/hr. Continue K⁺ replacement aggressively.
- Step 4: Consider bicarb ONLY if pH < 6.9 (give 100 mL of 8.4% NaHCO₃ in 400 mL sterile water over 2h). Controversial but ADA allows at pH < 6.9.
Key lesson: Always check K⁺ BEFORE starting insulin in DKA. K⁺ < 3.3 = replace first. This is the most dangerous moment in DKA management, insulin without adequate K⁺ kills.
| Drug | Dose / Route | Indication | Key Points |
|---|---|---|---|
| Regular Insulin | 0.14 units/kg/hr IV drip (no bolus) OR 0.1 units/kg/hr (with 0.1 units/kg IV bolus) ADA 2026 |
Insulin infusion | Do not start if K⁺ < 3.5. Reduce to 0.05 when BG < 250 |
| Normal Saline (0.9%) | 1–1.5 L over 1 hr, then 250–500 mL/hr | Volume resuscitation. LR is an acceptable alternative (SMART, 2018 -balanced crystalloids reduce AKI/death vs NS in critically ill) | Switch to 0.45%NS after initial bolus based on corrected Na⁺ |
| KCl | 20–40 mEq/hr IV (max 40 mEq/hr via central line) 10–20 mEq/hr peripheral |
Hypokalemia in DKA | Continuous cardiac monitoring. Expect K⁺ to drop as insulin given |
| Sodium Bicarbonate | 100 mEq in 400 mL D5W over 2 hrs | pH < 6.9 only | Controversial. May worsen hypokalemia and CNS acidosis. Use sparingly |
| Phosphate | 20–30 mmol IV over 6 hrs | PO₄ < 1.0 mg/dL with symptoms | Routine replacement not recommended. Risk of hypocalcemia |
| Glargine (Lantus) | 0.25–0.3 units/kg SQ (or prior home dose) | Transition off drip | Give 2 hours before stopping drip. Do not skip |
Patient: 24 y/o F with T1DM, ran out of insulin 3 days ago, presents with nausea, vomiting, abdominal pain, and Kussmaul breathing.
Key findings: HR 118, BP 98/62, RR 28. BG 480, pH 7.12, bicarb 6, AG 28, K⁺ 5.4, BHB 6.8 mmol/L.
Management:
- NS 1L bolus over 1h, then 0.45% NS at 250 mL/hr
- K⁺ 5.4 (>3.5), start regular insulin drip at 0.14 units/kg/hr (no bolus), OR alternatively 0.1 u/kg IV bolus + 0.1 u/kg/hr drip ADA, 2026
- Add KCl 20 mEq/L to each liter of IVF (total body K⁺ depleted despite normal serum K⁺)
- When BG < 250, add D5 to IVF and reduce insulin to 0.05 units/kg/hr
Teaching point: Serum K⁺ is artificially elevated due to acidosis-driven transcellular shift. Total body K⁺ is always depleted in DKA. Aggressively replete as insulin drives K⁺ intracellularly.
Patient: 58 y/o M with T2DM on empagliflozin and metformin, presents with 2 days of nausea, vomiting, and fatigue after a GI illness.
Key findings: BG 185, pH 7.22, bicarb 12, AG 22, BHB 5.2 mmol/L. K⁺ 4.1.
Management:
- Recognize euglycemic DKA, glucose near-normal but AG acidosis with ketones
- Hold SGLT2 inhibitor immediately
- Start insulin drip + D10 infusion (glucose already low, needs dextrose from the start)
- Volume resuscitate aggressively, SGLT2i causes osmotic diuresis
Teaching point: SGLT2 inhibitors mask hyperglycemia by enhancing renal glucose excretion. Always check ketones in SGLT2i users presenting with nausea/vomiting, even if glucose is normal.
Patient: 31 y/o F with T1DM, presenting with DKA triggered by UTI. Found altered in the ED.
Key findings: BG 520, pH 7.08, bicarb 5, AG 30, K⁺ 2.9, ECG shows U waves and prolonged QTc.
Management:
- DO NOT start insulin, K⁺ < 3.5 is an absolute contraindication
- Aggressive K⁺ repletion: KCl 40 mEq/hr IV via central line with continuous telemetry
- Start insulin ONLY when K⁺ ≥ 3.5 (recheck q1h during repletion)
- Treat UTI precipitant with appropriate antibiotics
Teaching point: Insulin before K⁺ repletion in hypokalemic DKA causes fatal arrhythmias. This is the single most important safety rule in DKA management.
- Glucose: every 1 hour (via POC meter)
- BMP (or at least K⁺, bicarb): every 2–4 hours
- Anion gap: calculated every 2–4 hours to confirm closure
- Beta-hydroxybutyrate: every 4 hours (preferred over urine ketones)
- Urine output: target ≥ 0.5 mL/kg/hr -place Foley if needed
- ECG: if K⁺ < 3.0 or > 6.0
- Stopping insulin too early -always wait for AG closure, not just BG normalization
- Forgetting the 2-hour overlap when transitioning to SQ insulin
- Overcorrecting fluids -iatrogenic fluid overload, especially in elderly or cardiac patients
- Missing the precipitant -always ask: why did they get DKA?
- Euglycemic DKA on SGLT2i -BG may be near-normal; check ketones regardless
- Cerebral edema -rare in adults but watch for headache, declining GCS during treatment
- Hypokalemia (from insulin shifting K⁺ intracellular)
- Hypoglycemia (from excess insulin or failure to add dextrose)
- Cerebral edema (especially children, rapid fluid shifts)
- ARDS (from aggressive fluid resuscitation)
- Thrombosis (hypercoagulable state)
- Patient tolerating PO fluids and meals
- On appropriate SQ insulin regimen
- BG < 200, AG closed, K⁺ repleted
- Precipitant identified and addressed
- Diabetes education arranged
- Endocrine follow-up within 1–2 weeks
 ⤢ Tap to open full size
⤢ Tap to open full size
Text version
- BG > 250 mg/dL
- pH < 7.3 / Bicarb < 18
- Anion gap > 10–12
- Ketones positive (serum BHB preferred)
- Euglycemic DKA: BG normal on SGLT2i
- Infection (30–40%)
- Missed insulin (20–25%)
- New diagnosis T1DM
- MI, pancreatitis, surgery
- SGLT2 inhibitor use
- BG every 1h (POC)
- BMP q2–4h
- Anion gap q2–4h
- BHB q4h
- UOP ≥ 0.5 mL/kg/hr
- Insulin with K⁺ < 3.5
- Stopping drip at BG normal
- Missing euglycemic DKA
- No SQ overlap
- Missing precipitant
- pH < 7.0 / bicarb < 10
- Altered mental status
- Hemodynamic instability
- K⁺ < 3.0 with ECG changes
- ADA 2026: No IV insulin bolus -drip only at 0.1 u/kg/hr
- Resolution: Gap closure, not glucose normalisation
- Bicarb: Only if pH < 6.9 (not routine)
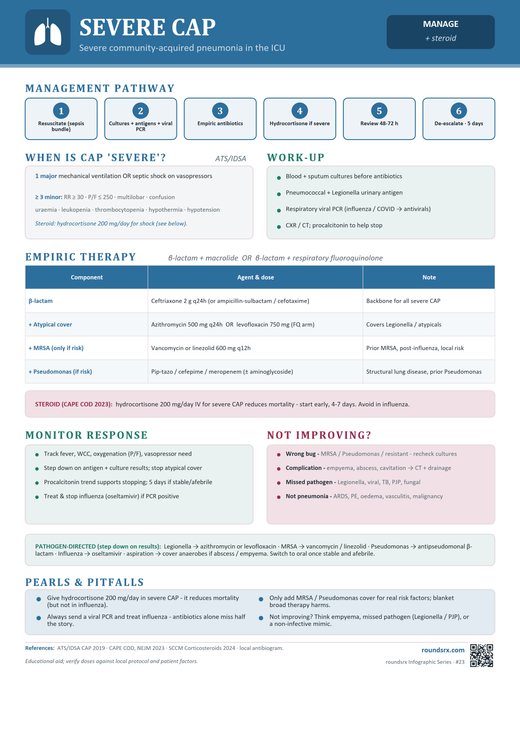
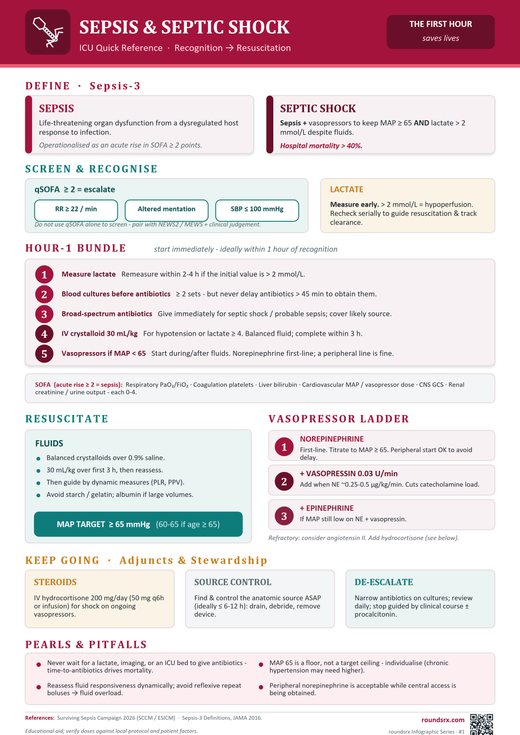
Sepsis & Septic Shock
Septic Shock: Sepsis + vasopressor requirement to maintain MAP ≥ 65 mmHg + serum lactate > 2 mmol/L despite adequate fluid resuscitation. In-hospital mortality > 40%.
⚠️ SSC 2026: qSOFA has poor sensitivity -misses too many septic patients. NEWS/MEWS now recommended as primary screening tools.
Replaced by Sepsis-3 (2016) due to poor specificity -SIRS is present in most hospitalized patients Sepsis-3, 2016 regardless of infection. Still used as a triage trigger in some institutions given its high sensitivity.
| Domain | 2021 SSC | 2026 SSC Update |
|---|---|---|
| Screening | qSOFA suggested outside ICU | NEWS/NEWS2/MEWS/SIRS now recommended OVER qSOFA. qSOFA has poor sensitivity -should not be sole screening tool. |
| Fluids | 30 mL/kg crystalloid within 3h. No preference NS vs balanced. | 30 mL/kg still suggested. Balanced crystalloids now suggested over 0.9% saline (except TBI). New: fluid removal after resuscitation now addressed. |
| Vasopressors | Start via central line. NE first-line (strong). | Peripheral vasopressor start now OK -don't delay for central access. NE still first-line but downgraded to conditional ("suggest"). New: MAP 60-65 for adults ≥ 65 years. |
| Steroids | Suggested if ongoing vasopressor need (reversed 2016 stance against routine steroids) | Maintained from 2021. Hydrocortisone 200 mg/day for septic shock with ongoing vasopressor requirement. No specific wait time mandated (trial enrollment used ≥ 4h). |
| Antibiotics | Within 1h of recognition | Refined: 1 hour for septic shock, 3 hours for sepsis without shock. New: antibiotic optimization & prehospital antibiotics may reduce mortality (OR 0.58). |
| Beta-lactam dosing | Not addressed | Recommend (strong) prolonged infusion of beta-lactams for maintenance after loading dose. Improves time-dependent killing. |
| Anaerobic coverage | Routine empiric pip-tazo / metronidazole as part of broad-spectrum cover | Stop reflexively adding anaerobic coverage. Chanderraj, 2024 showed empiric anti-anaerobic agents in critically ill patients without an anaerobic source ↑ mortality, C. diff, and VRE. New default empiric: Vanc + Cefepime. Add Zosyn / metronidazole only for clear anaerobic sources (intra-abdominal, aspiration w/ abscess, nec fasc, pelvic, bite wound). |
| Source | Frequency | Typical pathogens |
|---|---|---|
| Pulmonary (pneumonia) | ~40–50% | S. pneumoniae, K. pneumoniae, P. aeruginosa, MRSA, influenza, COVID-19 |
| Genitourinary | ~20–25% | E. coli, Klebsiella, Proteus, enterococci |
| Intra-abdominal | ~15–20% | Polymicrobial gram-negatives + anaerobes (B. fragilis); E. coli, enterococci. Sources: cholangitis, perforation, diverticulitis, abscess, ischemic bowel |
| Skin / soft tissue | ~5–10% | S. aureus (incl. MRSA), Group A strep, Clostridium. Includes necrotizing fasciitis, cellulitis, infected wounds, decubitus ulcers |
| Catheter / line / device | ~5% | CoNS, S. aureus, Candida, gram-negatives. CLABSI, infected hardware (pacemaker, prosthetic joint, VP shunt) |
| CNS, endocarditis, other | < 5% | Variable. CNS: S. pneumoniae, N. meningitidis, Listeria (elderly/immunocompromised). Endocarditis: S. aureus, viridans strep, enterococci. Consider early in sepsis with no clear source, especially with fever + AMS or new murmur |
| No source identified | ~10–15% | Empiric broad-spectrum coverage; reassess daily. Higher in immunocompromised (neutropenic fever, post-transplant). Consider occult abscess, fungal, viral, atypical organisms |
- Fever > 38.3°C OR hypothermia < 36°C (hypothermia = worse prognosis)
- Tachycardia, tachypnea
- Hypotension, warm/flushed skin (early distributive), later cold/mottled
- Altered mental status (confusion, agitation, lethargy)
- Decreased urine output (< 0.5 mL/kg/hr)
- Elevated lactate (tissue hypoperfusion marker)
- Measure serum lactate (repeat if initial > 2 mmol/L to confirm clearance)
- Blood cultures × 2 sets from 2 separate sites -before antibiotics, but do not delay antibiotics > 45 min waiting for cultures
- Broad-spectrum antibiotics administered IV, 1h for septic shock, 3h for sepsis without shock (SSC 2026)
- 30 mL/kg balanced crystalloid (LR or PlasmaLyte) bolus if MAP < 65 mmHg OR lactate ≥ 4 mmol/L (SSC 2026 suggests balanced over 0.9% saline, except TBI)
- Vasopressors if MAP < 65 despite fluid resuscitation → target MAP ≥ 65
- Lactate -venous or arterial; most critical early test; > 4 = cryptic shock regardless of BP
- Blood cultures × 2 peripheral sets (before antibiotics)
- BMP -creatinine (AKI), glucose, bicarb (metabolic acidosis)
- CBC with differential (leukocytosis, left shift, or leukopenia)
- Procalcitonin -helps guide antibiotic duration (de-escalation at < 0.25)
- UA + urine culture (UTI/urosepsis -2nd most common source)
- Sputum Gram stain + culture, respiratory panel (pneumonia -most common source)
- LFTs, lipase, RUQ ultrasound (abdominal source)
- Coagulation panel (PT/INR, PTT, fibrinogen) -if DIC suspected
- LP (cell count, protein, glucose, Gram stain, culture) if CNS source
- C. diff if recent antibiotics + diarrhea
- Bedside echo -cardiac function, IVC collapsibility (volume status), wall motion, pericardial effusion (fastest, most actionable)
- CXR -portable if unstable; pneumonia, pulmonary edema, effusion
- RUQ ultrasound -gallbladder, biliary dilation (cholangitis)
- CT abdomen/pelvis with contrast -abdominal source, abscess (do not delay abx for CT)
- CT head -if AMS, meningismus, focal neuro deficit (LP after if no mass lesion)
| Lactate Level | Category | Action |
|---|---|---|
| < 2 mmol/L | Normal | Standard care; monitor if clinical concern |
| 2–4 mmol/L | Elevated -sepsis | Aggressive resuscitation; repeat lactate in 2h |
| ≥ 4 mmol/L | Cryptic shock | Mandatory aggressive resuscitation: 30 mL/kg balanced crystalloid, ICU evaluation, source control, repeat lactate q2h. Vasopressors if MAP < 65 after fluids (per SSC 2026, not all cryptic shock requires immediate pressors if BP responds). |
▶ How to Escalate Sepsis Care, Step by Step (tap to expand)
| Criterion | What | Why |
|---|---|---|
| Sepsis (Sepsis-3) | Suspected infection + SOFA ↑ ≥ 2 (organ dysfunction) | Sepsis-3 dropped SIRS for SOFA because SIRS over-called and missed sicker patients. SOFA tracks 6 organ systems (resp, coag, hepatic, CV, CNS, renal). |
| Septic shock | Sepsis + MAP < 65 requiring pressors AND lactate > 2 despite adequate volume | Defines the "Hour-1 bundle" trigger. Mortality jumps from ~10% (sepsis) to ~40% (shock); the bundle window is when survival is shaped. |
| Bedside screen | qSOFA ≥ 2 (RR ≥ 22, AMS, SBP ≤ 100) or NEWS2 ≥ 5 at floor/ED | qSOFA is a screening trigger, not a diagnosis. A "0" qSOFA in a sick-looking patient still gets the workup, clinical gestalt overrides scores. |
| Action | How | Why |
|---|---|---|
| Lactate | VBG or specific lactate. Recheck in 2 hr. | Initial lactate stratifies severity; clearance > 10% per 2 hr is the resuscitation goal. Persistent lactate > 4 is high-mortality. |
| Cultures BEFORE antibiotics | 2 blood cultures from separate sites; site-specific (UA, sputum, CSF, peritoneal) as indicated. Don't delay antibiotics > 45 min for cultures. | Pretreatment cultures double yield. But never sacrifice antibiotic timing in shock, get what you can in < 45 min and move on. |
| Antibiotics within 1 hr (shock) or 3 hr (sepsis without shock) | Default empiric: vancomycin + cefepime. Tailor to source (see Step 3). | 2026 SSC moved off pip-tazo as universal default because of ACORN (2024, ↑ AKI when paired with vanc) and Chanderraj (2024, anti-anaerobic overuse → ↑ mortality, C. diff, VRE). Cefepime + vanc is broad without unnecessary anaerobes. |
| Balanced crystalloid 30 mL/kg | LR or PlasmaLyte (not NS) over 1-3 hr if MAP < 65 or lactate ≥ 4. Re-assess after each 500 mL (passive leg raise, lung auscultation, JVP). | SMART (2018): balanced fluids reduce major adverse kidney events vs NS. CLOVERS (2023): liberal vs restrictive fluid showed no benefit, don't reflex more if not responding. NS only in TBI. |
| Start pressors early | Norepinephrine 0.01-0.05 mcg/kg/min, titrate to MAP ≥ 65. Peripheral start is OK while central line is being placed, don't delay. | SSC 2026: peripheral pressors safe for short-term use, removing the "central access first" delay. Waiting for central line costs survival minutes. |
| Source | Empiric Regimen | Why |
|---|---|---|
| Unknown / undifferentiated | Vancomycin + cefepime | Default. Covers MRSA + Pseudomonas + GNR without unnecessary anaerobic spectrum. |
| Intra-abdominal, aspiration with abscess/empyema, nec fasc, pelvic, bite | Vancomycin + piperacillin-tazobactam, OR vanc + cefepime + metronidazole | Anaerobic coverage essential. Use pip-tazo despite AKI signal when the anaerobic indication is clear. |
| Pneumonia, severe community-acquired | Ceftriaxone + azithromycin (typical CAP), or vanc + cefepime if HAP/VAP risk | Macrolide for atypicals (Legionella, Mycoplasma). Add vanc if MRSA risk (post-influenza, cavitary, IVDU). |
| Urinary | Ceftriaxone (uncomplicated) or pip-tazo/cefepime (complicated, obstruction, hospital exposure) | ~70% E. coli, others Klebsiella, Pseudomonas. Add vanc only if hardware (stent, catheter) or known prior MRSA. |
| Meningitis | Ceftriaxone 2 g IV + vancomycin + dexamethasone (give before/with antibiotics in pneumococcal) + ampicillin (Listeria) if > 50 yr, immunocompromised, alcoholic, pregnant | Dexamethasone reduces mortality and neurologic sequelae in pneumococcal meningitis only when given before/with the first antibiotic dose (de Gans, 2002). |
| Neutropenic fever | Cefepime monotherapy (or pip-tazo). Add vanc only if hemodynamic instability, line infection, severe mucositis, MRSA history. | Routine empiric vanc no longer recommended (IDSA 2018, 2024 update); doesn't improve outcomes and selects resistance. |
| Suspected MRSA bacteremia / line infection | Vancomycin (AUC/MIC 400-600) ± gram-neg coverage; remove infected catheter | Vancomycin is the standard. Daptomycin if MIC ≥ 1.5 or persistent bacteremia. Linezolid for pulm if vanc trough not achievable. |
| Prior ESBL or MDR organism | Meropenem 1 g IV q8h | ESBL inactivates cefepime and pip-tazo unreliably; carbapenems are the standard. Reserve for clear indications to avoid carbapenem resistance. |
- Abscess → IR-guided or surgical drainage
- Necrotizing fasciitis → emergent surgical debridement (don't wait for imaging)
- Cholangitis / obstructive uropathy → urgent decompression (ERCP, percutaneous nephrostomy)
- Infected hardware (line, prosthetic joint, valve, device) → remove or replace
- Perforated viscus → emergent surgery
| Trigger | Do This | Why |
|---|---|---|
| NE ≥ 0.25-0.5 mcg/kg/min still not at MAP 65 | Add vasopressin 0.03 U/min fixed dose | VASST (2008): vasopressin spares NE; mortality signal in less-severe shock subgroup. Fixed dose, no titration. |
| Persistent shock on NE + vasopressin | Add epinephrine; consider hydrocortisone 200 mg/day IV (50 mg q6h or continuous) | APROCCHSS (2018): hydrocortisone + fludrocortisone reduced 90-day mortality. ADRENAL (2018): faster shock reversal without mortality benefit. SSC 2021/2026: conditional recommendation for ongoing vasopressor requirement. |
| Adequate MAP but cold extremities, rising lactate, low ScvO₂ | Add dobutamine 2-20 mcg/kg/min for low cardiac output | Cardiogenic component on top of distributive shock (sepsis cardiomyopathy). Echo to confirm low EF. |
| Lactate not clearing despite all above | Re-check source (missed undrained focus, persistent bacteremia), exclude β-agonist or metformin lactic acidosis, check echo | Persistent lactate after MAP and pressors are optimized usually means undrained source or wrong antibiotic. |
| Element | Target | Why |
|---|---|---|
| Lung-protective ventilation | TV 6 mL/kg IBW, Pplat ≤ 30, target SpO₂ 92-96% | ARDSNet (2000): TV 6 vs 12 mL/kg reduced mortality 22%. Applies to all ICU mechanical ventilation. |
| Glucose | 140-180 mg/dL | NICE-SUGAR (2009): tight control (81-108) increased mortality and 13× severe hypoglycemia. |
| DVT prophylaxis | Enoxaparin (UFH if CrCl < 30) + SCDs | Septic patients have high VTE risk. |
| Stress ulcer prophylaxis | PPI or H2-blocker IF mechanical ventilation > 48 hr, coagulopathy, prior GI bleed, TBI, large burns. Not universally. | SUP-ICU (2018): routine prophylaxis no mortality benefit; weigh C. diff and pneumonia risk. |
| Enteral nutrition | Within 24-48 hr | Preserves gut mucosal integrity. NUTRIREA-2 and CALORIES showed enteral and parenteral mortality similar but enteral has fewer complications. |
| Transfusion threshold | Hgb < 7 (or < 8 if active cardiac ischemia) | TRICC (1999): restrictive (< 7) non-inferior to liberal (< 10). |
- Narrow antibiotics to culture-directed therapy (e.g., vanc → cefazolin if MSSA; cefepime → ceftriaxone if susceptible).
- Stop empiric MRSA coverage if cultures negative at 48 hr and no MRSA risk factors.
- Total duration 5-7 days for most sepsis with good source control and clinical improvement (PRORATA, SAPS, BALANCE). Longer for endocarditis, osteo, undrained abscess, S. aureus bacteremia.
- Procalcitonin can guide stopping (PRORATA: 2.7 day reduction, no mortality penalty).
- De-resuscitate: once stable and MAP supported off pressors, start net-negative fluid balance. SSC 2026 explicitly added this. Fluid overload at day 3-5 worsens mortality.
| Scenario | Do This | Why |
|---|---|---|
| Severe penicillin allergy (anaphylaxis, SJS/TEN) | Aztreonam + vanc + metronidazole for broad coverage; meropenem if SJS to non-PCN beta-lactam | Cefepime is generally safe with non-severe PCN allergy (cross-reactivity ~1-3%), but in severe IgE/SJS history, aztreonam (monobactam) avoids cross-reactivity. |
| Renal failure / on dialysis | Avoid pip-tazo + vanc combo (ACORN AKI signal); use cefepime + vanc with AUC dosing; adjust all renally-cleared drugs | Vanc and beta-lactams need renal dose adjustment. Pip-tazo + vanc combo specifically raises AKI rate independent of baseline function. |
| Pregnancy | Cefepime, vancomycin, ceftriaxone are safe. Avoid tetracyclines, FQs, aminoglycosides, TMP-SMX (first trimester). | Standard category labels for these. Treat aggressively; sepsis in pregnancy carries high maternal-fetal mortality. |
| Sepsis-induced cardiomyopathy (drop in EF, cold extremities, low CO despite MAP) | Add dobutamine 2-20 mcg/kg/min while continuing NE | Septic cardiomyopathy is reversible, lasts days to weeks. Echo confirms; dobutamine supports CO until myocardium recovers. |
| Suspected adrenal crisis (hyponatremia, hyperkalemia, eosinophilia, on chronic steroids) | Empiric hydrocortisone 100 mg IV q8h upfront, before cosyntropin if life-threatening | Sepsis can precipitate adrenal crisis in chronic steroid users or unrecognized Addison. Stress-dose covers both relative adrenal insufficiency and sepsis itself. |
| Influenza or COVID superinfection suspected | Oseltamivir 75 mg BID or remdesivir/dexamethasone per current protocol; cover MRSA (post-influenza necrotizing pneumonia) and Strep pneumo | Post-influenza bacterial superinfection is classically MRSA (necrotizing) or pneumococcus. Don't withhold antiviral while bacterial workup pending. |
| Refractory shock + abdominal pain or distension | Urgent CT abdomen, surgical consult; consider mesenteric ischemia or perforated viscus | Missed surgical sources kill more than antibiotic choice. If shock won't budge, image and call surgery. |
| Cirrhosis with SBP | Ceftriaxone 2 g IV daily + albumin 1.5 g/kg day 1, 1 g/kg day 3 | Sort (1999): albumin reduces hepatorenal syndrome and mortality in SBP. Don't forget the albumin. |
| Heart failure or low EF on chronic GDMT | Hold ACEi/ARB/ARNI, MRA, SGLT2i during septic shock; continue cautiously after MAP supported and pressors weaning | Hemodynamic vulnerability in shock. SGLT2i specifically also raises euglycemic DKA risk in critical illness. |
| End-of-life / DNR with poor prognosis | Goals-of-care discussion early; palliative trajectory with antibiotics, analgesia, anti-secretory; avoid futile escalation | Septic shock in patients with poor baseline functional status has > 80% mortality. Aggressive ICU care without alignment to goals worsens dying. |
If shock criteria met (MAP < 65, lactate ≥ 4, AMS): activate ICU consult now -not after labs, not after imaging. Bedside echo to exclude obstructive shock (PE, tamponade) and assess LV function.
| Drug | Dose | Bugs Covered | ⚠️ Side Effects | When to Use |
|---|---|---|---|---|
| Piperacillin-tazobactam (Zosyn) | 3.375g IV q6h (or 4.5g q8h extended infusion over 4h) | Gram-positives: Strep, MSSA (not MRSA) Gram-negatives: E. coli, Klebsiella, Proteus, Pseudomonas, Enterobacter Anaerobes: Bacteroides, Fusobacterium | ⚠️ ↑ AKI when paired with vancomycin ACORN, 2024 (use cefepime + vanc as default empiric unless anaerobic source). C. diff (higher than cefepime, broad anaerobic kill). Hypokalemia (common, often missed, check daily BMP; mechanism = non-reabsorbable anion in distal tubule). Thrombocytopenia & neutropenia with courses > 7–14 days. Rash; DRESS (rare); cross-reactivity with severe PCN allergy. Transaminitis; cholestasis with prolonged infusion. False-positive serum galactomannan (critical in heme/onc aspergillus screening). Drug fever. Seizures in renal failure (rare). Diarrhea (non-C. diff). | Reserve for clear anaerobic source (intra-abdominal, aspiration w/ abscess, nec fasc, pelvic, bite wound). No longer the default empiric in 2026, Chanderraj, 2024 showed empiric anti-anaerobic agents without an anaerobic indication ↑ mortality, C. diff, and VRE. |
| Cefepime (Maxipime) | 2g IV q8h | Gram-positives: Strep, MSSA (not MRSA) Gram-negatives: E. coli, Klebsiella, Pseudomonas, Enterobacter, Serratia, Citrobacter No anaerobes | ⚠️ Cefepime-induced neurotoxicity (CIN), encephalopathy, confusion, myoclonus, asterixis, tremor, non-convulsive status epilepticus. Esp. renal failure, elderly, sepsis. Often misdiagnosed as ICU delirium; EEG shows triphasic waves or generalized periodic discharges. Resolves with discontinuation ± HD. Dose-adjust aggressively for CrCl. Overt seizures (part of spectrum). C. diff. Rash; hypersensitivity (PCN cross-reactivity ~1–3%, safe in non-severe PCN allergy). Thrombocytopenia, eosinophilia, positive Coombs (rare AIHA). Transaminitis. Drug fever; infusion-site phlebitis. Candidiasis / thrush with prolonged use. | New 2026 default empiric (paired with vanc). Covers Pseudomonas + GNR without anaerobic spectrum. ↓ AKI vs pip-tazo+vanc. Add metronidazole only if a true anaerobic source is identified. |
| Meropenem (Merrem) | 1g IV q8h | Gram-positives: Strep, MSSA (not MRSA) Gram-negatives: E. coli, Klebsiella, Pseudomonas, Enterobacter, ESBL-producers, Acinetobacter Anaerobes: Bacteroides | ⚠️ Seizures (esp. renal failure, CNS lesion, elderly, high dose, lower risk than imipenem; always dose-adjust for CrCl). ↓ valproic acid 50–90% in 24–48h → breakthrough seizures/status epilepticus (AVOID combo, dose-escalating VPA does NOT rescue; bridge to levetiracetam). C. diff, diarrhea, nausea. Rash / hypersensitivity (PCN cross-reactivity ~1%, safe in non-severe PCN allergy). Thrombocytosis, eosinophilia, positive Coombs (rare AIHA); transaminitis. VRE + Candida superinfection with prolonged courses. Encephalopathy/myoclonus in renal failure. | Use if: prior ESBL/MDR organism, recent hospitalization + IV abx within 90 days, high local resistance, failed pip-tazo. Broadest gram-negative coverage. |
| Vancomycin (Vancocin) | 15–20 mg/kg IV q8–12h (AUC/MIC target 400–600) | Gram-positives only: MRSA, MSSA, Strep, Enterococcus (not VRE) No gram-negatives. No anaerobes. | ⚠️ Nephrotoxicity / AKI (dose- and duration-dependent; worse with pip-tazo ACORN, 2024; AUC/MIC 400–600 guided dosing ↓ risk vs trough-only). Vancomycin flushing syndrome (formerly "Red Man", histamine release, NOT IgE allergy; infuse over ≥ 1h, pre-treat with antihistamine if recurrent). Ototoxicity (dose/duration; additive with loops + aminoglycosides). DRESS, SJS/TEN (rare). Linear IgA bullous dermatosis. Neutropenia + thrombocytopenia with courses > 7–14 days. Drug fever. Phlebitis, prefer central line for prolonged courses. | Add for MRSA coverage -any sepsis with: prior MRSA, IVDU, skin/soft tissue source, healthcare exposure, HD catheter. Pair with pip-tazo, cefepime, or meropenem. |
| Linezolid (Zyvox) | 600 mg IV/PO q12h | Gram-positives only: MRSA, VRE, Strep, Enterococcus No gram-negatives. No anaerobes. | ⚠️ Thrombocytopenia (courses > 7–14d, monitor CBC weekly; most common dose-limiting toxicity). Serotonin syndrome (weak reversible MAOi, avoid SSRIs, SNRIs, tramadol, meperidine, TCAs; ideally 2-week washout. Classic inpatient pimp trap). Peripheral neuropathy + optic neuritis (courses > 28d, may be irreversible; discontinue at first sign). Myelosuppression / pancytopenia (marrow suppression, > 14d). Lactic acidosis (mitochondrial protein synthesis inhibition, prolonged use, often > 28d). Tyramine reaction (avoid aged cheese, cured meats, wine, MAOi effect). Hypoglycemia in diabetics on sulfonylureas/insulin. Headache, nausea, diarrhea, rash. | Alternative to vanc if: CKD/AKI (no renal adjustment), VRE suspected, MRSA pneumonia (superior lung penetration), no IV access (100% PO bioavailability). |
| Metronidazole (Flagyl) | 500 mg IV q8h | Anaerobes: Bacteroides fragilis, Clostridium, Fusobacterium, Prevotella Protozoa: C. diff (PO), Giardia, Entamoeba | ⚠️ Disulfiram-like reaction with alcohol (flushing, tachycardia, nausea, vomiting, counsel: NO alcohol during + 72h after. Applies to mouthwash, cough syrup, IV meds in propylene glycol). Peripheral neuropathy (dose- and duration-related, distal axonal, courses > 4–6 weeks; may be irreversible). CNS toxicity, encephalopathy, cerebellar syndrome (ataxia, dysarthria, nystagmus), seizures. MRI: symmetric cerebellar dentate / corpus callosum splenium lesions; reversible with discontinuation. Metallic taste + nausea (very common, adherence issue). Warfarin INR ↑ (CYP2C9 inhibition, recheck INR at 48–72h; anticipate dose reduction). Lithium toxicity. Reversible leukopenia. Optic neuropathy (rare). Aseptic meningitis (very rare). | Add to cefepime or meropenem when anaerobic coverage needed (intra-abdominal, abscess, aspiration with empyema). Not needed with pip-tazo (already covers anaerobes). |
After initial bolus: reassess after each 500 mL. Check JVP, lung auscultation, passive leg raise response. Do not reflexively give more fluids if no hemodynamic response -start vasopressors. Fluid overload in sepsis = worse outcomes. CLOVERS, 2023 showed no benefit to liberal fluid strategy, supporting a conservative approach. Use crystalloids over colloids -CRISTAL, 2013 found no 28-day mortality difference between colloids and crystalloids. Notably, FEAST, 2011 demonstrated that fluid boluses increased mortality in febrile children (resource-limited setting), underscoring the importance of judicious fluid use.
Add vasopressin 0.03 units/min (fixed dose, no titration) when NE reaches 0.25–0.5 mcg/kg/min (spares NE, possibly reduces mortality) VASST 2008.
Add epinephrine for refractory shock. Use dobutamine (2–20 mcg/kg/min) only if MAP adequate but persistent signs of low CO (cold extremities, rising lactate, low ScvO₂).
Hydrocortisone 200 mg/day IV (50 mg q6h or continuous) for septic shock with ongoing vasopressor requirement (SSC 2021/2026 -conditional recommendation). Shortens shock duration. ADRENAL 2018; APROCCHSS 2018 CORTICUS, 2008.
Drain abscess (IR-guided or surgical). Remove infected IV lines (replace in new site). Decompress biliary obstruction (ERCP or percutaneous). Surgical consult for perforated viscus, necrotizing fasciitis, infected prosthetic. Time to source control should be < 6–12 hours for drainage procedures.
Glucose: Target 140–180 mg/dL with insulin infusion NICE-SUGAR, 2009. Avoid hypoglycemia.
DVT prophylaxis: Enoxaparin (or UFH if CrCl < 30) + SCDs.
Stress ulcer prophylaxis: IV PPI or H2-blocker if high-risk (mechanically ventilated > 48h, coagulopathy, history of GI bleed, TBI, burns > 35% BSA). Not all ICU patients need it -SUP-ICU, 2018: no mortality benefit from routine prophylaxis; weigh risk of C. difficile and nosocomial pneumonia.
Nutrition: Early enteral nutrition within 24–48h. Enteral is preferred over parenteral -NUTRIREA-2, 2018 and CALORIES, 2014 showed no mortality difference between parenteral and enteral, but enteral maintains gut integrity.
Antibiotic de-escalation: Reassess at 48–72h based on cultures + clinical trajectory. Target 5–7 days total if good source control and clinical improvement. Use procalcitonin to guide stopping PRORATA 2010.
| Parameter | Target | Notes |
|---|---|---|
| MAP | ≥ 65 mmHg (60-65 if age ≥ 65) | Higher (≥ 75) in chronic hypertension or AKI. SSC 2026: lower target 60-65 for older adults spares vasopressor exposure. |
| Lactate | Clearance ≥ 10% per 2h | Target < 2 mmol/L; failure to clear = reassess |
| UOP | ≥ 0.5 mL/kg/hr | Oliguria = inadequate perfusion or AKI |
| ScvO₂ | ≥ 70% | Low = high O₂ extraction → low CO or anemia |
| Glucose | 140–180 mg/dL | Avoid hypoglycemia -check q1–2h |
| Hgb | ≥ 7–9 g/dL | Transfuse if Hgb < 7 (or < 8 if cardiac ischemia) TRICC, 1999 |
- No anaerobic source → no anti-anaerobic agent. Routine empiric pip-tazo, metronidazole, or clindamycin in critically ill patients without an anaerobic indication is associated with higher mortality, C. difficile, and VRE. Chanderraj, 2024
| Clinical Scenario | Empiric Regimen | Notes |
|---|---|---|
| Sepsis, no clear source (default while workup pending) | Cefepime (Maxipime) 2g IV q8h (Pseudomonas, E. coli, Klebsiella, Enterobacter, MSSA) + Vancomycin (Vancocin) 25–30 mg/kg loading (MRSA, Strep, Enterococcus) | New 2026 default. Covers MRSA + Pseudomonas + GNR without unnecessary anaerobic coverage. Use this instead of Vanc + Zosyn unless an anaerobic source is identified. |
| CAP (community-acquired pneumonia) Pulmonary source = ~40–50% of sepsis | Ceftriaxone (Rocephin) 1–2g IV daily + Azithromycin (Zithromax) 500 mg IV/PO | Typical organisms (S. pneumoniae, H. influenzae) + atypicals (Mycoplasma, Legionella). Add vanc if MRSA risk (post-influenza, cavitary, prior MRSA). Levofloxacin monotherapy is an alternative. |
| Severe CAP + sepsis / HAP / VAP | Cefepime (Maxipime) 2g IV q8h + Vancomycin (Vancocin) | Pseudomonas + MRSA coverage. Cefepime preferred over Zosyn (2026), pneumonia is not an anaerobic source unless aspiration with abscess or empyema. |
| Urosepsis (community-acquired) GU source = ~20–25% of sepsis | Ceftriaxone (Rocephin) 1–2g IV daily | E. coli is #1 (~80%). Urinary tract is not an anaerobic source. Adjust by Gram stain + culture. Add ampicillin if Enterococcus on Gram stain. Cefepime if Pseudomonas risk (recurrent UTI, indwelling catheter, prior Pseudomonas). |
| Biliary / intra-abdominal source Abdominal source = ~15–20% of sepsis (perforation, peritonitis, cholangitis, diverticulitis, abscess) | Pip-tazo (Zosyn) 4.5g IV q6h OR Ceftriaxone + Metronidazole (Flagyl) 500 mg IV q8h | True anaerobic source. Anaerobic coverage is appropriate here. Urgent source control (ERCP, IR drainage, surgery) is as critical as antibiotics. |
| SBP (cirrhosis + ascites) | Ceftriaxone (Rocephin) 2g IV daily | SBP is monomicrobial GNR (E. coli, Klebsiella), does NOT need anaerobic coverage. If healthcare-associated SBP or recent broad abx: cefepime or meropenem. |
| Cellulitis (admitted, severe, non-necrotizing) Skin/soft tissue source = ~5–10% of sepsis | Vancomycin (Vancocin) (MRSA) + Cefepime only if GNR risk or unstable | Not an anaerobic infection. Most non-necrotizing cellulitis is Group A strep + S. aureus. Vanc alone is often sufficient. Skip Zosyn unless polymicrobial features. |
| Aspiration pneumonia with lung abscess, empyema, or witnessed large-volume aspiration | Ampicillin-sulbactam (Unasyn) 3g IV q6h OR Pip-tazo (Zosyn) 4.5g IV q6h | Routine "aspiration" CAP does NOT need anaerobic coverage. Reserve for clear anaerobic features: abscess, empyema, putrid sputum, severe dental disease, witnessed aspiration of gastric contents. |
| Neutropenic fever (ANC < 500) | Cefepime (Maxipime) 2g IV q8h ± Vancomycin | Cefepime monotherapy is the standard. Add vanc only for: hemodynamic instability, line infection, skin/soft tissue source, severe mucositis, or known MRSA colonization. Add micafungin at day 4–5 if persistent fever. |
| Suspected meningitis CNS source = < 5% of sepsis | Ceftriaxone (Rocephin) 2g IV q12h + Vancomycin + Dexamethasone (Decadron) 0.15 mg/kg IV q6h × 4d | Dex before or with first abx dose. Add ampicillin 2g IV q4h for Listeria if > 50yo, immunocompromised, or pregnant. Add acyclovir if HSV encephalitis suspected. |
| Necrotizing fasciitis | Vancomycin + Pip-tazo (Zosyn) 4.5g IV q6h + Clindamycin (Cleocin) 900 mg IV q8h | Polymicrobial soft tissue → anaerobes appropriate. Clindamycin = toxin suppression (50S inhibition), not for coverage. Surgical emergency, debridement ASAP. |
| Suspected fungal sepsis | Micafungin (Mycamine) 100 mg IV daily OR Fluconazole (Diflucan) 800 mg IV load → 400 mg daily | Risk factors: TPN, prior broad-spectrum abx, abdominal surgery, Candida colonization, persistent fever despite antibiotics. Micafungin preferred empirically (broader Candida coverage). Step down to fluconazole if C. albicans confirmed susceptible. |
| Known prior MDR organism (prior ESBL/CRE culture, MDR colonization, or local antibiogram > 10–20% ESBL) | Meropenem (Merrem) 1g IV q8h (ESBL, AmpC, Pseudomonas) + Vancomycin (Vancocin) (MRSA) | Reserve carbapenems for documented resistant organisms or high institutional ESBL prevalence. Add micafungin if Candida risk (TPN, lines, abdominal surgery). |
- Intra-abdominal, perforation, peritonitis, abscess, cholangitis, diverticulitis, ischemic bowel
- Aspiration pneumonia with clear risk, poor dentition, lung abscess, empyema, witnessed large-volume aspiration. Routine CAP-aspiration does NOT need anaerobes.
- Necrotizing soft tissue infection, gas-forming, polymicrobial, Fournier's
- Female pelvic, PID, tubo-ovarian abscess, septic abortion, postpartum endometritis
- Oropharyngeal / dental / head & neck, Ludwig's angina, deep neck space infection, odontogenic abscess
- Bite wounds, human or animal
| Agent | Dose | Receptor | Role | Avoid |
|---|---|---|---|---|
| Norepinephrine (Levophed) 1ST LINE | 0.01–3 mcg/kg/min | α₁>>β₁ | First-line. ↑ SVR + mild inotropy | - |
| Vasopressin (Pitressin) ADD-ON | 0.03 units/min (fixed, no titration) | V1/V2 | Add vasopressin when NE dose reaches 0.25–0.5 mcg/kg/min (per SSC 2026). Adding vasopressin early allows NE dose reduction (NE-sparing effect). May reduce AKI (V2-mediated water reabsorption). Non-catecholamine → works even in catecholamine-resistant shock (acidosis, downregulated adrenergic receptors). VASST 2008 SSC 2026 | Cardiac ischemia (coronary vasospasm), mesenteric ischemia at high doses, hyponatremia (V2 effect -monitor Na⁺) |
| Epinephrine (Adrenalin) 2ND LINE | 0.01–0.5 mcg/kg/min | α₁, β₁, β₂ | Refractory shock. Adds inotropy. | Falsely elevates lactate (β₂ effect) |
| Phenylephrine (Neo-Synephrine) | 0.5–6 mcg/kg/min | α₁ pure | If tachyarrhythmia limits NE | Low CO states (pure vasoconstriction) |
| Dobutamine (Dobutrex) | 2–20 mcg/kg/min | β₁>β₂ | Low CO despite adequate MAP | Without vasopressor if MAP < 65 |
| Dopamine (Intropin) AVOID | - | D1, β₁, α₁ | Avoid in sepsis -more arrhythmias, higher mortality SOAP II, 2010 | Avoid |
| Drug | Indication | Dose | Evidence |
|---|---|---|---|
| Hydrocortisone (Solu-Cortef) | Septic shock with ongoing vasopressor requirement (SSC 2021/2026 -conditional) | 200 mg/day IV (50 mg q6h or continuous) | ADRENAL 2018 -faster shock reversal; APROCCHSS 2018 -mortality benefit with hydrocort + fludrocort |
| Drotrecogin alfa | - | Withdrawn from market | PROWESS-SHOCK 2012 -no benefit |
| Clinical Scenario | Why This Empiric | Culture Result | De-Escalate To | Duration |
|---|---|---|---|---|
| Sepsis, no clear source most common starting point | Vanc + Cefepime, covers MRSA + Pseudomonas + GNR. No anaerobic source → no Zosyn (2026). | Blood cx: MSSA | Stop both. → Cefazolin 2g IV q8h | Bacteremia: 2–4 weeks |
| Sepsis, no clear source | Vanc + Cefepime, broadest non-anaerobic empiric | Blood cx: MRSA | Stop cefepime. Continue Vancomycin (AUC-guided) | Min 2 weeks, longer if endocarditis |
| Fever + tachycardia (unclear source) very common, often turns out to be SIRS, not sepsis | Vanc + Cefepime, empiric for possible sepsis without anaerobic source | All cx negative at 48h. PCT < 0.25. Improving. | Stop all antibiotics. Consider non-infectious SIRS? | Stop if no infection identified |
| CAP (standard) Pulmonary source = ~40–50% of sepsis | Ceftriaxone + Azithro, standard CAP: typicals + atypicals | Legionella urinary antigen positive | Stop ceftriaxone. Continue Azithromycin 500mg IV/PO daily alone (or levofloxacin) | 5 days (azithro) or 7 days (levo) |
| Severe CAP + sepsis | Vanc + Zosyn, severity warranted broad coverage beyond standard CAP regimen | Sputum: S. pneumoniae (pan-sensitive). MRSA swab neg. | Stop vanc (NPV > 95%). Zosyn → Ceftriaxone 1g IV daily → PO amoxicillin when afebrile | 5 days total (PCT-guided) |
| Urosepsis GU source = ~20–25% of sepsis | Vanc + Cefepime, empiric until source confirmed (no anaerobes, urinary tract is not an anaerobic source) | Urine cx: E. coli (pansensitive) | Stop both. → Ceftriaxone 1g IV daily → PO cipro or TMP-SMX | UTI: 5–7 days. Pyelo: 7–10 days |
| Pyelonephritis + sepsis | Ceftriaxone 1g IV daily, first-line for community-acquired urosepsis (GNR coverage) | Urine: E. coli (susceptible to cipro + TMP-SMX) | IV → PO ciprofloxacin 500mg BID or TMP-SMX DS BID when afebrile + tolerating PO | 7 days total |
| Perforated appendicitis (post-op) Abdominal source = ~15–20% of sepsis | Zosyn 3.375g IV q6h, GNR + anaerobe coverage for abdominal source | Intra-abdominal: E. coli + Bacteroides (susceptible) | Continue Zosyn → PO amox-clav 875/125 q12h when tolerating PO | 4 days post source control STOP-IT, 2015 |
| SBP (cirrhosis + ascites) | Ceftriaxone 2g IV daily, SBP is monomicrobial GNR (E. coli, Klebsiella). Not polymicrobial → does NOT need anaerobic coverage. If healthcare-associated SBP or recent abx: cefepime or meropenem. | Ascitic fluid cx: E. coli. Susceptible to ceftriaxone. | Continue ceftriaxone. | 5 days. Repeat paracentesis at 48h, PMN should drop > 25%. |
| Cellulitis (admitted, severe) Skin/soft tissue source = ~5–10% of sepsis | Vanc + Cefepime, MRSA + GNR. Non-necrotizing cellulitis is NOT an anaerobic infection, skip Zosyn (2026). | Blood cx negative at 48h. No abscess. Non-purulent. | Stop both. → PO cephalexin 500mg q6h. If purulent: TMP-SMX DS BID | 5 days |
| HAP/VAP | Vanc + Cefepime, hospital-acquired = Pseudomonas + MRSA risk. Cefepime preferred over Zosyn (2026), pneumonia is not an anaerobic source unless aspiration with abscess/empyema. | Sputum: Pseudomonas aeruginosa (susceptible to cefepime) | Stop vanc. Continue Cefepime 2g IV q8h | 7 days for HAP/VAP |
| Line sepsis (suspected CLABSI) | Vanc + Cefepime, MRSA + GNR coverage for line infection (line is not an anaerobic source) | Blood cx: Coag-negative Staph (1 of 2 bottles) | Likely contaminant. 1 bottle + improving + no hardware → stop vanc. If 2/2 bottles or prosthetic → treat. | Contaminant: stop. True: 5–7 days (no hardware) or 4–6 wks (prosthetic) |
| Neutropenic fever | Vanc + Cefepime, cefepime = anti-pseudomonal monotherapy for febrile neutropenia; vanc if line infection suspected | Blood cx: Enterococcus faecalis (ampicillin-susceptible) | Stop both. → Ampicillin 2g IV q4h | 2–4 weeks (rule out endocarditis with TTE/TEE) |
| Neutropenic fever (no source found) | Vanc + Cefepime, standard febrile neutropenia regimen | All cx negative at 72h. ANC recovering (> 500). | Stop antibiotics when afebrile × 48h + ANC > 500 × 2 days | Stop with ANC recovery. |
| Sepsis + prior ESBL on antibiogram uncommon, modifier based on prior cultures | Meropenem + Vanc, known ESBL colonization requires carbapenem empirically | Blood cx: ESBL E. coli | Stop vanc. Continue meropenem. IV → PO TMP-SMX if susceptible for step-down | 7–14 days (source-dependent) |
| Sepsis + TPN/central line + prior abx | Vanc + Cefepime + Micafungin, Candida risk factors (TPN, lines, broad abx). No anaerobic source → cefepime, not Zosyn. | Blood cx: Candida albicans (fluconazole-susceptible) | Stop vanc + cefepime. Micafungin → Fluconazole 400mg IV/PO daily. Remove all central lines. | 14 days from first negative blood cx |
| VAP + prior meropenem use | Meropenem + Vanc, prior carbapenem use selects for resistant organisms | Sputum: Stenotrophomonas maltophilia | Stop meropenem (intrinsically resistant). → TMP-SMX 15mg/kg/day IV divided q6-8h | 10–14 days. Meropenem selects for Steno. |
| Necrotizing fasciitis rare, surgical emergency | Vanc + Zosyn, broadest empiric for polymicrobial soft tissue infection | Wound cx: Group A Strep | Stop both. → Penicillin G 4MU IV q4h + Clindamycin 900mg IV q8h (toxin suppression) | Until debridement complete + clinical improvement |
Patient: 78 y/o F with DM2 and CKD3, presents with confusion, dysuria, and fever 39.2°C for 1 day.
Key findings: HR 112, BP 108/68, RR 24. Lactate 4.2, WBC 18.4K, Cr 2.8 (baseline 1.6), UA positive for nitrites and leukocyte esterase.
Management:
- Blood cultures x2 drawn, then ceftriaxone 1g IV within 1 hour SSC, 2026
- 30 mL/kg LR bolus (lactate ≥ 4 = mandatory resuscitation)
- Repeat lactate at 2h, clearance ≥ 10% is the target
- CT abdomen to rule out renal abscess or obstruction
Teaching point: Cryptic shock, lactate ≥ 4 with normal blood pressure. This patient meets septic shock criteria even though MAP is adequate. Do not be falsely reassured by a normal BP when lactate is elevated.
Patient: 62 y/o M with COPD, presents with productive cough and fevers. CXR shows RLL consolidation. MAP 52 after 2L LR.
Key findings: HR 128, RR 32, SpO₂ 88% on 6L NC. Lactate 6.8, WBC 22K, procalcitonin 14.5.
Management:
- Norepinephrine via peripheral IV, do not delay for central line CENSER, 2019
- Cefepime 2g IV q8h + vancomycin 25 mg/kg load (pneumonia is not an anaerobic source, SSC 2026 / Chanderraj, 2024 prefers cefepime over Zosyn)
- NE at 0.3, MAP still 58, add vasopressin 0.03 u/min VASST, 2008
- Hydrocortisone 50 mg IV q6h (ongoing vasopressor-dependent shock) ADRENAL, 2018
Antibiotic Stewardship: Day 2, sputum culture grows S. pneumoniae (pan-sensitive). MRSA nasal swab negative (NPV > 95%). De-escalate: stop vancomycin, narrow cefepime → ceftriaxone 1g IV daily. Check PCT trend, if ≥ 80% decline from peak, target 5-day total course.
Teaching point: Vasopressor escalation: NE first → vasopressin second (fixed 0.03 u/min) → hydrocortisone if still requiring high-dose pressors. Wean NE first, vasopressin last. Always reassess antibiotics at 48-72h when cultures finalize.
Patient: 55 y/o F, admitted with severe CAP and sepsis. Started on cefepime + vancomycin empirically (SSC 2026, pneumonia is not an anaerobic source).
Key findings: Admission PCT 8.2. Blood cultures grow pan-sensitive S. pneumoniae. MRSA nasal swab negative. Day 3: PCT 1.4 (83% decline), afebrile x24h.
Management:
- De-escalate vancomycin (MRSA swab negative, NPV > 95%)
- Narrow cefepime to ceftriaxone (culture-directed for S. pneumoniae)
- PCT ≥ 80% decline, stop antibiotics at day 5 PRORATA, 2010
- Total duration: 5 days (not the traditional 7-14)
Antibiotic Stewardship: Culture-directed narrowing is the goal. MRSA swab negative → stop vancomycin. Pan-sensitive organism → narrow to simplest effective agent. PCT-guided stop rule avoids unnecessary antibiotic days, fewer C. diff, less resistance, shorter stay.
Teaching point: Procalcitonin-guided de-escalation safely reduces antibiotic duration by 2-3 days. Stop rule: PCT < 0.25 or ≥ 80% decline from peak. Every unnecessary antibiotic day increases C. diff and resistance risk.
Patient: 78F from nursing home, altered mental status, T 39.2°C, HR 112, BP 82/48, WBC 22k. Foley catheter in place. UA: positive nitrites, leukocyte esterase, bacteria.
Key findings: Lactate 4.8 mmol/L → septic shock.
Management:
- Blood cultures × 2 + urine culture BEFORE antibiotics
- Cefepime 2g IV within 1 hour (covers Pseudomonas, catheter-associated UTI risk). Add vancomycin if concerned for MRSA bacteremia.
- 30 mL/kg LR bolus. Reassess after each liter.
- Norepinephrine via peripheral IV, don't wait for central line SSC, 2026
Antibiotic Stewardship: Day 2, urine culture grows E. coli (pan-sensitive). Narrow cefepime → ceftriaxone 1g IV daily. Plan transition to PO ciprofloxacin or TMP-SMX for discharge. Total course: 7-10 days for complicated UTI.
Teaching point: Catheter-associated UTI + septic shock = remove the catheter (source control), cover Pseudomonas empirically, start pressors early, and narrow at 48h when cultures return.
Patient: 55M with diabetes, rapidly spreading erythema on left leg × 12 hours. Pain out of proportion to exam. Crepitus on palpation. T 39.8°C, HR 125, BP 95/58, WBC 28k, lactate 5.2.
This is a surgical emergency, NOT a medical one.
- Do NOT wait for LRINEC score if clinical suspicion is high. Pain out of proportion + crepitus + sepsis = OR now.
- Vancomycin + pip-tazo + clindamycin (clindamycin inhibits toxin production in Group A Strep)
- Emergent surgical consult → radical debridement within hours. Every hour of delay ≈ +7.6% mortality.
- Expect return to OR every 24–48h for re-exploration until margins are clean.
Antibiotic Stewardship: Post-debridement, wound cultures guide narrowing. If Group A Strep confirmed → narrow to penicillin G + clindamycin (toxin suppression). If polymicrobial → maintain broad coverage. Duration guided by clinical response, not a fixed number of days.
Teaching point: Nec fasc is a surgical disease with medical support. The antibiotic that matters most is the scalpel. Call surgery BEFORE imaging.
- Cultures finalized? → Narrow antibiotics today if possible. What day of antibiotics are we on?
- Lactate cleared? → < 2 on two consecutive measurements = adequate perfusion
- Vasopressor trajectory → Weaning or escalating? Note exact dose and trend
- UOP adequate? → Target ≥ 0.5 mL/kg/hr. If oliguric -reassess volume status + pressor dose
- Source controlled? → Drain placed? Infected line removed? Surgery consulted?
- Procalcitonin trend → Falling PCT supports antibiotic cessation PRORATA 2010
- Glucose 140–180 mg/dL? → Avoid hypoglycemia; tight control not beneficial NICE-SUGAR, 2009
- DVT prophylaxis ordered? Stress ulcer prophylaxis (SUP) indicated? Updated (SCCM/ASHP, 2024): SUP only if coagulopathy (PLT <50K, INR >1.5), shock (on vasopressors), or chronic liver disease. Vent alone is no longer a clear indication. Enteral feeding is protective, if tolerating feeds, SUP is likely unnecessary. Discontinue when risk factors resolve.
- Nutrition started? → Enteral preferred within 24–48h if hemodynamically stable
- Sedation/delirium assessment → CAM-ICU, RASS target, daily SAT/SBT
| Parameter | Frequency | Target / Action |
|---|---|---|
| MAP (arterial line) | Continuous | ≥ 65 mmHg; higher if chronic HTN |
| Urine output | Hourly | ≥ 0.5 mL/kg/hr; oliguria = reassess volume + pressors |
| Lactate | q2h until < 2 × 2 | Target clearance ≥ 10%/2h |
| Blood glucose | q1–2h (insulin infusion) | 140–180 mg/dL; avoid < 70 |
| BMP | q6–12h initially | Monitor AKI (creatinine), electrolytes, bicarb |
| CBC | Daily | Thrombocytopenia = DIC; trend WBC |
| Cultures | At 48–72h | De-escalate antibiotics based on growth + sensitivities |
| Procalcitonin | q48–72h | If falling and < 0.25 → consider stopping antibiotics PRORATA 2010 |
| Coags (INR, fibrinogen, D-dimer) | Daily if coagulopathy | Fibrinogen < 1.5 + falling = DIC |
| Temperature | Continuous | Hypothermia = worse prognosis than fever |
Certain infections require longer: endocarditis (4–6 weeks), osteomyelitis (6 weeks -oral step-down is acceptable OVIVA, 2019), S. aureus bacteraemia (minimum 14 days from first negative culture).
 ⤢ Tap to open full size
⤢ Tap to open full size
Text version
- Sepsis: SOFA ≥ 2 + suspected infection
- Septic shock: Vasopressors + lactate > 2 despite IVF
- qSOFA: AMS + RR ≥ 22 + SBP ≤ 100 (≥ 2 = high risk, screen only)
- SIRS: ≥ 2 of temp >38/<36, HR >90, RR >20, WBC >12k/<4k (historical, high sensitivity triage)
- Lactate ≥ 4 = cryptic shock even if BP normal
- 🫁 Pulmonary ~40–50% (pneumonia)
- 🚿 GU ~20–25% (urosepsis)
- 🫀 Intra-abdominal ~15–20%
- 🩹 Skin/soft tissue ~5–10%
- 💉 Line / device ~5%
- 🧠 CNS / endocarditis < 5%
- ❓ No source identified ~10–15%
- Delaying antibiotics for cultures
- Using dopamine SOAP II, 2010
- NS over balanced crystalloids
- No source control
- Broad abx never narrowed
- Missing hypothermia = bad sign
Acute Decompensated Heart Failure
| Profile | Perfusion | Congestion | Management |
|---|---|---|---|
| Warm & Wet (~70%) | Adequate (warm extremities, normal mentation) | Yes (JVD, edema, crackles) | IV diuresis. This is the most common profile. Furosemide, monitor UOP, daily weights. |
| Cold & Wet (~20%) | Impaired (cold, clammy, AMS, low UOP) | Yes | ICU. Inotropes (dobutamine/milrinone) + diuresis. May need invasive monitoring. Consider mechanical circulatory support (MCS) early. |
| Cold & Dry (~5%) | Impaired | No | Cardiogenic shock. Pressors + inotropes + MCS. See Cardiogenic Shock topic. |
| Warm & Dry (~5%) | Adequate | No | Compensated. Optimize oral GDMT. Do NOT over-diurese. Symptom management. |
- Dyspnea, orthopnea, paroxysmal nocturnal dyspnea
- Rapid weight gain (> 2 kg in 48 hrs)
- Leg edema, fatigue, decreased exercise tolerance
- JVD, S3 gallop, pulmonary crackles, pitting edema
- Elevated JVP = elevated filling pressures (wet)
- Cool extremities, narrow pulse pressure = low output (cold)
| Test | Why |
|---|---|
| BNP / NT-proBNP | Most sensitive. Very high NPV for ruling out HF. BNP > 400 or NT-proBNP > 900 supports ADHF. |
| CXR | Pulmonary vascular congestion, Kerley B lines, cardiomegaly, pleural effusions. Fastest imaging. |
| Echo | Definitive. EF (HFrEF vs HFpEF), wall motion abnormalities, valvular disease, pericardial effusion. |
| BMP | Cr (tracks with diuresis), Na⁺ (hyponatremia = poor prognosis), K⁺, bicarb. |
| Troponin | Rule out ACS as trigger. Demand ischemia common in ADHF. |
| ECG | STEMI trigger? Afib with RVR? New LBBB? |
| CBC, LFTs, TSH | Anemia worsens HF. Congestive hepatopathy. Thyroid disease is reversible cause. |
- Medication non-adherence -most common, especially diuretics and sodium restriction
- Dietary indiscretion -sodium/fluid overload
- ACS / ischemia -always rule out with troponin + ECG
- Afib with RVR -loss of atrial kick + tachycardia-mediated worsening
- Uncontrolled HTN -flash pulmonary edema
- Infection / sepsis -increased metabolic demand on failing heart
- Worsening renal function -impaired diuresis
- Anemia, thyroid disease, PE, medication changes (NSAIDs, CCBs, TZDs)
| Drug (Brand) | Dose | Role | Key Notes |
|---|---|---|---|
| Furosemide (Lasix) 1ST LINE | 40–200 mg IV bolus or 10–40 mg/hr infusion | First-line diuretic. Decongestion. | 1–2.5× home oral dose IV. Monitor UOP, K⁺, Mg, Cr daily. Continuous infusion may cause less ototoxicity than large boluses. |
| Bumetanide (Bumex) ALTERNATIVE | 1–4 mg IV | Alternative loop diuretic. 40:1 ratio (furosemide 40 mg ≈ bumetanide 1 mg). | More predictable oral bioavailability than furosemide. Some prefer in outpatient setting. |
| Metolazone (Zaroxolyn) ADD-ON | 2.5–10 mg PO 30-60 min before loop diuretic | Sequential nephron blockade. Overcomes diuretic resistance. | Thiazide-like. Works even at low GFR (unlike HCTZ). Massive electrolyte shifts -monitor K⁺, Mg, Na aggressively. |
| Chlorothiazide (Diuril) ADD-ON (IV) | 500–1000 mg IV 30 min before loop diuretic | IV thiazide for sequential nephron blockade. Use when NPO or fast onset needed. | Only IV thiazide in US. Onset 15 min, duration 6–12h. Fails below eGFR 30 (unlike metolazone). Expensive (~$40–80 per dose). Severe hypokalemia, hyponatremia -monitor K⁺, Mg, Na aggressively. Dose BEFORE the loop, never after. |
| Acetazolamide (Diamox) ADD-ON | 500 mg IV daily × 3 days | Proximal tubule block (carbonic anhydrase inhibitor). Add-on for diuretic resistance and when metabolic alkalosis develops from loop diuresis. | ADVOR, 2022: successful decongestion at day 3 42% vs 30% (12% absolute increase, NNT < 9; RR 1.46) when added to loop. Works upstream of the loop so it stacks with thiazide (different site). Watch for metabolic acidosis (expected from mechanism) and hypokalemia. Dose-reduce at low eGFR. |
| Tolvaptan (Samsca) AQUARETIC / NICHE | 15–30 mg PO daily (inpatient start only) | V2 receptor antagonist (aquaretic). Excretes free water only, no Na effect. For hypervolemic hyponatremia (Na < 125) when further diuresis would worsen sodium. | EVEREST, 2007: symptom and weight benefit, no mortality benefit. Must start inpatient -rapid Na correction risk (ODS). Avoid in cirrhosis (hepatotoxicity). Short-term bridge only. |
| Nitroglycerin (Tridil) HYPERTENSIVE ADHF | 5–200 mcg/min IV drip | Preload reduction. Rapid relief of dyspnea in flash pulmonary edema with SBP > 140. | Venodilator predominantly. Titrate to symptom relief. Avoid if SBP < 90, severe AS, RV infarct, or PDE5 inhibitor use (sildenafil within 24h). |
| Nitroprusside (Nipride) SPECIALIZED | 0.3–5 mcg/kg/min IV | Afterload + preload reduction. Refractory hypertensive ADHF. | Requires arterial line. Cyanide toxicity risk > 48h or > 2 mcg/kg/min. Thiocyanate levels if prolonged. Avoid in renal failure (thiocyanate accumulation). |
| Dobutamine (Dobutrex) COLD & WET | 2–20 mcg/kg/min IV | Inotrope for low-output state. Cold & Wet profile. | ↑ CO, ↑ HR. Never use alone if MAP < 65 -pair with NE. Tachyphylaxis after 72h. See Inotropes Guide. |
| Milrinone (Primacor) COLD & WET / RV | 0.125–0.75 mcg/kg/min IV (skip loading dose) | Inodilator. RV failure, pulmonary HTN, patients on chronic BB. | ↓ PVR (key advantage in RV failure). Renally cleared -dose-adjust in AKI. Longer half-life (2–3h) than dobutamine's ~2 min. |
| Norepinephrine (Levophed) 1ST LINE PRESSOR | 0.05–1 mcg/kg/min IV (titrate to MAP ≥ 65) | First-line vasopressor for hypotension or cardiogenic shock complicating ADHF. Pair with dobutamine or milrinone if low CO. | SOAP II, 2010: preferred over dopamine (fewer arrhythmias, better cardiogenic shock outcomes). Central line preferred (extravasation necrosis risk peripherally). Once pressors needed, hold ACEi/ARB/ARNI, BB, MRA, SGLT2i until off pressors. |
| Ferric carboxymaltose (Injectafer) INPATIENT IRON | 15 mg/kg IV (max 750 mg/dose) × 2 doses separated by ≥ 7 days | Iron repletion in iron-deficient HF. Give during admission, not outpatient, for maximum event reduction. | AFFIRM-AHF, 2020: 26% reduction in HF hospitalizations at 52 weeks. Criteria: ferritin < 100 OR ferritin 100–299 + TSAT < 20%. Screen every ADHF admission. Avoid in active infection. Rare anaphylaxis (safer than older iron dextran). |
| Drug Class | During ADHF | When to Hold |
|---|---|---|
| ACEi / ARB / ARNI* *ARNI = Angiotensin Receptor-Neprilysin Inhibitor (sacubitril-valsartan) | Continue unless hypotensive or AKI | SBP < 90, Cr rising > 30%, K⁺ > 5.5 |
| Beta-blocker | Reduce dose if decompensated. Do NOT stop abruptly. | Cardiogenic shock, symptomatic bradycardia, severe hypotension |
| MRA* (spironolactone) *MRA = Mineralocorticoid Receptor Antagonist (spironolactone, eplerenone) | Continue if K⁺ stable | K⁺ > 5.0, AKI |
| SGLT2i* *SGLT2i = Sodium-Glucose Co-Transporter 2 Inhibitor (dapagliflozin, empagliflozin) | Continue if tolerated. EMPULSE, 2022: empagliflozin started in-hospital ADHF → clinical benefit. | eGFR < 20, DKA risk |
- HOLD: ACEi / ARB / ARNI, beta-blocker, MRA, SGLT2i, nitrates, hydralazine
- START: norepinephrine for MAP, plus dobutamine for low CO (milrinone preferred if RV failure or pulmonary HTN)
- CONTINUE (at adjusted dose): loop diuretic, titrated to UOP and MAP. Decongestion is still needed, just carefully.
- Resume sequentially once off pressors, MAP stable > 65, and Cr not rising: ACEi/ARB first, then beta-blocker, then MRA, then SGLT2i. Titrate back to home doses before discharge.
| Drug Class | Why it comes off | Notes |
|---|---|---|
| NSAIDs STOP | Prostaglandin inhibition blunts loop diuretic response, drives AKI, increases HF hospitalizations. | Includes ibuprofen, naproxen, ketorolac, diclofenac, and COX-2 inhibitors (celecoxib). Use acetaminophen or adjuvants for pain. |
| Non-DHP CCBs (diltiazem, verapamil) STOP in HFrEF | Negative inotropy worsens HF exacerbation. Contraindicated in HFrEF. | Amlodipine and felodipine are the only CCBs considered safe in HFrEF. Non-DHPs are OK in HFpEF when rate control is needed. |
| Thiazolidinediones (pioglitazone, rosiglitazone) STOP | PPAR-γ activation drives Na and water retention. Increased HF hospitalization; contraindicated in NYHA III-IV. | Switch diabetes management to SGLT2i or GLP-1 RA (both reduce HF events). |
| Saxagliptin HOLD / SWITCH | SAVOR-TIMI 53 showed an increased HF hospitalization signal. Sitagliptin and linagliptin appear safer. | Switch to sitagliptin, or better, to SGLT2i or GLP-1 RA. |
| Pregabalin / gabapentin HOLD | Peripheral edema is common and can mimic or worsen HF volume overload. | Especially hold if edema is disproportionate to the congestion picture. Consider duloxetine or TCA for neuropathic pain. |
| High-dose glucocorticoids MINIMIZE | Mineralocorticoid activity at high doses drives Na and water retention, HTN. | Not always possible to stop (autoimmune disease). Use lowest effective dose. Hydrocortisone has less mineralocorticoid effect at replacement doses. |
| Anti-arrhythmics with negative inotropy (flecainide, propafenone, disopyramide) AVOID in HFrEF | Class IC agents increase mortality in structural heart disease (CAST). Disopyramide is negatively inotropic. | Amiodarone and dofetilide are the only rhythm-control agents considered safe in HFrEF. |
| Excess IV fluids STOP | Overzealous maintenance fluids or high-Na medication carriers undo diuresis. Reconcile total Na and volume intake daily. | Convert IV meds to concentrated formulations. Use D5W as carrier when a drip is essential. |
- Step 0: Address reversible causes first. Stop NSAIDs (prostaglandin inhibition blunts loop response). Treat hypotension (kidneys can't diurese if MAP is too low, may need pressors to perfuse them). Switch PO to IV when gut edema is present. Check TSH (hypothyroid fluid retention mimics resistance). Consider bilateral renal artery stenosis if ACE-induced AKI pattern.
- Step 1: Max the loop. Double the IV dose (up to 200 mg furosemide IV bolus), switch from PO to IV, or start a continuous infusion (10-40 mg/hr). Gut edema makes PO absorption unreliable, so IV is the default in ADHF.
- Step 2: Add a tubular co-blocker (sequential nephron blockade). Two options at different tubular sites that can be used alone or stacked: thiazide (metolazone PO or Diuril IV) blocks the distal tubule, and acetazolamide 500 mg IV daily × 3 blocks the proximal tubule. ADVOR 2022: acetazolamide added to loop produced successful decongestion in 42% vs 30% at day 3 (12% absolute increase, NNT < 9; RR 1.46). Acetazolamide is particularly useful when loop diuresis has caused metabolic alkalosis. Give the thiazide 30-60 min before the loop.
- Step 3: Start an SGLT2 inhibitor if not already on one. Dapagliflozin 10 mg PO or empagliflozin 10 mg PO. EMPULSE / EMPAG-HF 2022: in-hospital start during ADHF reduced weight, NT-proBNP, and clinical events. Also foundational GDMT with mortality benefit. Drop the loop dose ~25% when starting to avoid over-diuresis.
- Step 4: Albumin + furosemide sandwich if serum albumin < 2.5 g/dL. See full breakdown at the bottom of this section.
- Step 5: Tolvaptan if hypervolemic AND hyponatremic (Na < 125). Blocks ADH at the collecting duct so the kidney excretes free water only, no Na effect. Must start inpatient (rapid-correction risk). Avoid in liver disease. EVEREST 2007 showed symptom and weight benefit without mortality benefit.
- Step 6: Ultrafiltration or dialysis if all pharmacologic options fail and the patient remains volume-overloaded with AKI or refractory acidosis.
| Feature | Furosemide (Lasix) | Chlorothiazide (Diuril) | Metolazone (Zaroxolyn) |
|---|---|---|---|
| Class | Loop | Thiazide (IV only in US) | Thiazide-like (PO only) |
| Role | Primary diuretic | Add-on for resistance | Add-on for resistance |
| Site of action | Thick ascending limb (NKCC2) | Distal tubule (NCC) | Distal tubule (NCC) |
| Route | IV or PO | IV only | PO only |
| Typical dose | 20-200+ mg IV | 500-1000 mg IV | 2.5-10 mg PO |
| Onset | IV 5 min / PO 30 min | IV 15 min | PO 60 min |
| Duration | ~2 h | 6-12 h | 12-24 h (longest) |
| % filtered Na blocked (alone) | ~25% (most potent single agent) | ~3-5% | ~5% |
| Works at eGFR < 30? | Yes | No | Yes (unique among thiazides) |
| Cost per dose | Pennies | ~$40-80 | Pennies |
| Main toxicities | Hypokalemia, hypomagnesemia, ototoxicity (high dose / rapid push), pre-renal AKI | Severe hypokalemia, hyponatremia, hypomagnesemia | Same as Diuril but longer and more profound (24h action window) |
| One-liner | The engine | Fast IV turbo | Long-acting PO turbo |
- Patient can swallow, any eGFR: metolazone 2.5-10 mg PO 30-60 min before the loop. Default choice. Cheap, long-acting, works in advanced CKD.
- NPO, or need fast predictable onset: Diuril 500-1000 mg IV 30 min before the loop. Works in 15 min. Expensive. Fails below eGFR 30.
- eGFR < 30: metolazone is the only option. Diuril and HCTZ lose efficacy at this level of renal function.
- Reaching for Diuril when metolazone PO would work. Diuril is expensive ($40-80 per dose vs pennies for metolazone) and shorter-acting. If the patient can swallow and isn't in fulminant gut edema, metolazone is the default.
- Giving the thiazide after or with the loop. The synergy depends on the thiazide being at the distal tubule BEFORE the loop dumps Na downstream. Dose the thiazide 30-60 min first, every time.
| Drug | Dose | Mechanism | When to reach for it |
|---|---|---|---|
| Acetazolamide (Diamox) ADVOR 2022 | 500 mg IV daily × 3 days | Proximal tubule carbonic anhydrase inhibitor. Blocks Na/HCO₃ reabsorption upstream of the loop. | Added to loop in ADHF → 46% more successful decongestion at day 3. Especially useful when loop diuresis has caused metabolic alkalosis. Can stack with thiazide (different site). |
| Dapagliflozin / Empagliflozin GDMT + DIURESIS | Dapa 10 mg PO / Empa 10 mg PO daily | Proximal tubule SGLT2 block. Modest natriuresis plus mortality/HF-hospitalization benefit independent of diabetes. | Start in-hospital during ADHF if not already on one. EMPULSE / EMPAG-HF 2022 showed reduced weight, NT-proBNP, clinical events. Drop loop ~25% to avoid over-diuresis. |
| Tolvaptan (Samsca) NICHE | 15-30 mg PO daily (inpatient start only) | V2 receptor antagonist (aquaretic). Blocks ADH at collecting duct. Excretes free water only, no Na effect. | Hypervolemic AND hyponatremic (Na < 125) when further diuresis would worsen sodium. Liver toxicity limits long-term use. Avoid in cirrhosis. |
| Hypertonic saline + high-dose furosemide NICHE / EU | 3% saline 150 mL + furosemide 250-500 mg IV, BID | Tonicity gradient mobilizes interstitial Na back into the vascular space, so the loop has more Na to excrete. | Refractory HF failing standard escalation. More European than US practice. SMAC-HF 2011. Avoid if Na > 140. |
- NSAIDs (including ketorolac), prostaglandin inhibition blunts loop response. Stop them.
- Hypotension, kidneys can't diurese below a perfusion threshold. MAP < 65 may need pressor support before more diuretic.
- Gut edema, PO furosemide bioavailability drops dramatically. Switch to IV.
- Hypothyroidism, fluid retention mimics volume overload. Check TSH.
- Bilateral renal artery stenosis, ACE-induced AKI looks like diuretic resistance. Consider if Cr jumps on ACEi/ARB with diuretic.
- Non-adherence to sodium restriction, ask the family what the patient is actually eating.
- Hypoalbuminemia < 2.5, impairs loop delivery to its tubular target (see sandwich, Step 4).
- "Renal-dose dopamine" (1-3 mcg/kg/min), no benefit. ROSE-HF 2013 was the definitive nail in the coffin. Don't order it.
- Nesiritide (recombinant BNP), ASCEND-HF 2011 neutral on outcomes, increases hypotension. Abandoned in most centers.
- Aggressive fluid restriction in cardiogenic shock, the kidneys need perfusion pressure. Restricting fluid here worsens AKI without improving congestion.
- Oncotic pull. Albumin raises plasma oncotic pressure, mobilizing interstitial fluid back into the vascular space so the loop has volume to diurese.
- Drug delivery. Furosemide is ~95% albumin-bound. In hypoalbuminemia, less drug reaches the proximal tubule for active secretion, so less reaches its NKCC2 target. Supplementing albumin restores drug delivery to the thick ascending limb.
- Diuretic-resistant edema despite max loop + thiazide
- Serum albumin < 2.5 g/dL
- Nephrotic syndrome with anasarca
- Cirrhotic refractory edema
- ICU third-spacing / capillary leak
- Post-op volume overload with low albumin
- Albumin 25% 100 mL IV (25 g) over 30 min
- Then furosemide 40-80 mg IV push at the end of the infusion
- Repeat q6-12h if needed
Patient: 68 y/o M with HFrEF (EF 25%), presenting with 10-lb weight gain, orthopnea, and bilateral leg edema. Home furosemide 80 mg PO BID.
Key findings: JVP 14 cm, bibasilar crackles, 3+ pitting edema. BNP 3,200, Cr 1.6 (baseline 1.2), K⁺ 3.2.
Management:
- IV furosemide 160 mg bolus (2x home oral dose), monitor UOP, target > 200 mL in 2h
- UOP 80 mL in 2h, double to 320 mg IV, add metolazone 5 mg PO 30 min prior
- Continue GDMT: SGLT2i safe in-hospital EMPULSE, 2022
- Replete K⁺ aggressively (target > 4.0), daily weights and strict I/Os
Teaching point: Diuretic resistance requires dose escalation (ceiling effect), then sequential nephron blockade with metolazone. A Cr bump ≤ 0.3 is acceptable during active diuresis.
Patient: 72 y/o F with HFrEF (EF 15%), presents with confusion, cool mottled extremities, and anasarca. SBP 78.
Key findings: MAP 52, narrow pulse pressure, lactate 4.1, Cr 3.2 (baseline 1.4), BNP 8,400. Echo: EF 12%.
Management:
- ICU admission, cold and wet profile (low CO + congestion)
- Start dobutamine 5 mcg/kg/min to improve cardiac output before diuresis
- Once MAP improves, add IV furosemide for decongestion
- Reduce BB dose but do NOT discontinue abruptly
Teaching point: Cold and wet is the most dangerous profile. These patients need inotropes before diuresis, you cannot diurese a heart that is not generating adequate forward flow.
Patient: 58 y/o M, no cardiac history, 1 week of progressive dyspnea with new AF and RVR (HR 152).
Key findings: JVP 12 cm, S3 gallop, BNP 2,800. Echo: EF 30%, dilated LV, moderate MR.
Management:
- Rate control with IV amiodarone (avoid diltiazem in HFrEF, negative inotrope)
- IV furosemide 40 mg (diuretic-naive starting dose)
- Initiate all 4 GDMT pillars: ARNI + BB + MRA + SGLT2i PARADIGM-HF, 2014
- Anticoagulation for AF, coronary angiogram to rule out ischemic etiology
Teaching point: Tachycardia-mediated cardiomyopathy from uncontrolled AF is reversible with rate/rhythm control. Start all 4 GDMT pillars early, do not wait to titrate one before starting the next.
Patient: 58M with newly diagnosed HFrEF (EF 25%), BP 118/72, HR 78, K⁺ 4.2, Cr 1.1. Currently on no cardiac medications.
🔄 Old approach: Start ACEi → wait weeks → add BB → wait weeks → add MRA → months later maybe ARNI. Patients spent months without full therapy.
New approach (2022 AHA/ACC, STRONG-HF, 2022): Start all 4 pillars within 1–2 weeks at low doses. Don't wait for one to reach target before starting the next.
| Timepoint | Action |
|---|---|
| Day 1 (Admission) | SGLT2i: Dapagliflozin (Farxiga) 10mg daily -start immediately, no titration needed, minimal BP effect. Easiest pillar to add on day 1. |
| Day 2–3 | ARNI: Sacubitril-valsartan (Entresto) 24/26mg BID -if SBP > 100 and off pressors. Go straight to ARNI (skip ACEi if new diagnosis). If already on ACEi, must wash out 36h before starting ARNI. Check BMP: K⁺ and Cr before adding MRA. |
| Day 3–5 (once near-euvolemic, off pressors) | Beta-blocker: Carvedilol (Coreg) 3.125mg BID -start low. Do NOT start during active decompensation or on inotropes (risk of cardiogenic shock). Wait until diuresis has taken effect and hemodynamics are stable. MRA: Spironolactone (Aldactone) 25mg daily -if K⁺ < 5.0 and eGFR > 30. |
| All 4 pillars on board within 1 week. Now uptitrate in parallel: | |
| Week 2 | Entresto → 49/51mg BID, carvedilol → 6.25mg BID (if BP and HR tolerate). |
| Week 4 | Entresto → 97/103mg BID (target dose), carvedilol → 12.5mg BID. |
| Week 8 | Carvedilol → 25mg BID (target dose). |
Key principles:
- Each drug reduces mortality independently -every day without full GDMT is a missed opportunity.
- Hypotension (SBP < 90) is the main limiting factor -prioritize ARNI > BB > MRA if BP-limited.
- "Creatinine bumps" of 0.3–0.5 are acceptable when starting RAAS inhibitors -don't reflexively stop.
- SGLT2i + MRA together are safe -monitor K⁺ but the risk of hyperkalemia is lower than feared.
Patient: 64F with known HFrEF (EF 20%), presents with orthopnea, PND, bilateral crackles, JVP 14cm, 2+ pitting edema. BP 142/88, SpO₂ 90% on RA.
Profile: Wet & Warm (congested, adequate perfusion) -most common presentation.
Immediate:
- Sit upright, O₂ to maintain SpO₂ > 92%. BiPAP if respiratory distress.
- Furosemide (Lasix) 80mg IV push (give 2× their home oral dose as IV dose -she takes 40mg PO daily → give 80mg IV; can escalate to 100mg / 2.5× if prior dose was inadequate). Can redose in 2h if < 100mL UOP.
- If inadequate response: double the dose → 160mg IV. If still inadequate → add metolazone (Zaroxolyn) 5mg PO 30 min before next lasix dose (sequential nephron blockade).
Monitoring: Strict I&Os, daily weights (goal: net negative 1–2L/day), BMP BID (watch K⁺ and Cr -"creatinine bumps" of 0.3–0.5 are acceptable if patient is decongesting).
Home GDMT: Continue metoprolol succinate (Toprol XL) at current dose (do NOT uptitrate during decompensation, but do NOT stop unless cardiogenic shock). Hold ACEi/ARNI if hypotensive or Cr rising sharply.
Discharge when: Stable on oral diuretics × 24h, ambulatory SpO₂ > 92%, weight at or near dry weight, scheduled HF clinic follow-up within 7 days.
| Parameter | Frequency | Target / Action |
|---|---|---|
| Daily weights | Every morning, same scale, before breakfast | Target 1-2 kg/day net loss during active diuresis. Weight gain > 2 lbs/day = fluid retention → uptitrate diuretics. |
| Strict I&Os | Every shift (q8h tallies) | Net negative 1-2 L/day during active diuresis. UOP ≥ 0.5 mL/kg/hr. If UOP drops, consider diuretic dose increase or combination diuretic therapy. |
| BMP (K⁺, Cr, Na⁺) | Daily while on IV diuretics; q1-2 days after RAAS inhibitor initiation or titration | K⁺ 4.0-5.0 (RAAS inhibitors raise K⁺, diuretics lower it). Cr rise ≤ 0.3 acceptable with diuresis. Na < 130 → consider fluid restriction. |
| Blood pressure | q4-6h inpatient; each clinic visit outpatient | SBP ≥ 90 for ARNI/ACEi/ARB titration. Tolerate asymptomatic SBP 90-100 if on GDMT. Hold vasodilators if symptomatic hypotension. |
| Heart rate | q4-6h inpatient; each visit outpatient | Resting HR 60-70 on maximally tolerated beta-blocker. Do NOT uptitrate BB during active decompensation. |
| BNP / NT-proBNP | Admission and pre-discharge (trend) | > 30% reduction from admission = adequate decongestion. Discharge BNP predicts readmission risk. |
| Echocardiogram (EF) | Reassess at 3-6 months after GDMT optimization | EF improvement on GDMT may reclassify HFrEF → HFimpEF. Continue all GDMT even if EF improves. |
| Telemetry | Continuous during IV diuresis and inotrope use | Monitor for AF, VT, bradycardia from BB/digoxin. Discontinue when stable on oral regimen. |
| Functional status | Each assessment | Dyspnea improvement, orthopnea resolution, exercise tolerance, appetite. The exam matters more than the labs. |
| Test | Rationale | Key Values |
|---|---|---|
| BNP / NT-proBNP | Diagnosis and prognostication. Trend to assess treatment response. | BNP >400 pg/mL or NT-proBNP >900 pg/mL (age <75) supports HF. Obesity falsely lowers BNP. Full high/low breakdown ↓ |
| TTE (echocardiogram) | Classify HFrEF (EF ≤40%) vs HFpEF (EF ≥50%). Assess wall motion, valves, diastolic function, RVSP. | EF ≤40% = HFrEF. EF 41–49% = HFmrEF. LA dilation, elevated E/e′ suggest elevated filling pressures. |
| BMP | Cr (cardiorenal syndrome), K⁺ (before RAAS inhibitors), Na⁺ (hyponatremia = poor prognosis), bicarb | Cr rise >0.3 from baseline = cardiorenal. Na <135 = independent mortality predictor. |
| CBC | Anemia worsens HF (high-output physiology). Infection as precipitant. | Hgb <10 → evaluate and treat anemia. Leukocytosis → infectious trigger? |
| Iron studies | Iron deficiency (even without anemia) worsens HF outcomes. IV iron improves symptoms. | Ferritin <100 OR ferritin 100–299 + TSAT <20% = iron deficient. Treat with IV iron FAIR-HF, 2009. |
| TSH | Hyper- and hypothyroidism are reversible causes of HF. | Check in all new HF diagnoses. |
| ECG | Ischemia, arrhythmia (new AF), LVH, LBBB (CRT candidacy if QRS ≥150 ms). | LBBB + EF ≤35% + QRS ≥150 ms → strong CRT indication. |
| Troponin | Rule out ACS as trigger for decompensation. Chronic mild elevation common in HF. | Acute rise-and-fall → ACS workup. Chronic low-level elevation = myocardial stress (not necessarily ACS). |
| CXR | Pulmonary edema (cephalization, Kerley B lines, effusions), cardiomegaly. | ~20% of ADHF patients have a normal CXR. Do not rely on CXR alone to rule out HF. |
| Condition | Why it raises BNP |
|---|---|
| Cardiac (the signal you want) | |
| Heart failure (HFrEF and HFpEF) | Volume and pressure overload stretch the ventricular wall, the intended diagnostic signal. Degree of elevation tracks severity and prognosis. |
| Atrial fibrillation | Atrial stretch plus the rapid ventricular rate raise BNP independent of HF, so new AF can push BNP into the “HF range” and muddy the diagnosis. Interpret cautiously in AF. |
| ACS / myocardial ischemia | Ischemic wall stress and stunning raise BNP; a high BNP post-MI predicts higher HF and mortality risk (prognostic, not just diagnostic). |
| Valvular disease (AS, MR) | Chronic pressure (AS) or volume (MR) load stretches the ventricle even before symptoms; rising BNP can flag the time for intervention. |
| Myocarditis, cardiac contusion, post-cardiac surgery, post-cardioversion | Direct myocardial injury or stress releases BNP transiently. |
| Non-cardiac (raises BNP without HF, the traps) | |
| Older age | BNP rises with age regardless of HF. Use age-adjusted NT-proBNP cutoffs: <450 (age <50), <900 (50–75), <1800 (>75) pg/mL to rule in acute HF. |
| CKD / renal failure | Reduced clearance raises baseline levels. NT-proBNP is affected more than BNP because NT-proBNP is cleared only by the kidney. Use higher cutoffs in CKD and trend rather than relying on a single value. |
| Pulmonary embolism | Acute RV pressure overload stretches the right ventricle; an elevated BNP in PE marks RV strain and worse prognosis (risk-stratification, not diagnosis). |
| Pulmonary hypertension, cor pulmonale, severe COPD | Chronic RV pressure overload stretches the RV, raising BNP from the right side of the heart. |
| Sepsis / critical illness | Cytokine-mediated myocardial depression plus volume shifts raise BNP; very common in the ICU and a frequent reason a BNP is hard to interpret there. |
| Female sex | Higher baseline BNP than men at any given age, a population effect to keep in mind near cutoffs. |
| Anemia, high-output states (cirrhosis, hyperthyroidism) | Increased cardiac work and circulating volume raise wall stress and therefore BNP. |
| Condition | Why BNP is low despite real HF |
|---|---|
| Obesity (especially BMI >35) | Adipocytes express natriuretic peptide clearance receptors (NPR-C), so BNP is cleared faster and runs low. A “normal” BNP does not rule out HF in an obese patient, consider halving the cutoff (roughly 50 pg/mL). NT-proBNP is less affected. |
| Flash (hyperacute) pulmonary edema | In the first 1–2 hours (e.g., hypertensive flash edema) BNP has not had time to rise. A low early value does not exclude acute HF, recheck a few hours later. |
| HFpEF vs HFrEF | Lower ventricular wall stress in HFpEF means lower BNP for the same degree of congestion; a meaningful minority of acute HFpEF presents with near-normal BNP. |
| Constrictive pericarditis / tamponade | The constrained ventricle cannot stretch, so BNP stays lower than the congestion suggests. Useful discriminator: BNP is markedly lower in constrictive pericarditis than in restrictive cardiomyopathy, which helps tell the two apart. |
| Stable, compensated chronic HF on optimal therapy | Lower wall stress than during decompensation, BNP falls toward the patient’s “dry” baseline. Trend against that personal baseline, not a population cutoff. |
- Use NT-proBNP if the patient is on sacubitril/valsartan (ARNI, Entresto), the hard rule. Neprilysin inhibition blocks BNP breakdown so BNP is falsely elevated and uninterpretable; NT-proBNP is not a neprilysin substrate and stays valid.
- NT-proBNP also has the edge for sample stability (half-life ~1–2 h vs BNP ~20 min, less minute-to-minute noise) and has well-validated age-adjusted rule-in cutoffs (>450 if <50y, >900 if 50–75, >1800 if >75).
- Lean BNP in advanced CKD, both rise with renal impairment but NT-proBNP rises more (renal-only clearance), so BNP is marginally less confounded. Soft preference, both still need adjusted cutoffs.
- Never compare a BNP value to an NT-proBNP value, NT-proBNP runs roughly 5–10× higher. Pick one assay and trend that same one across the admission and between visits.
- CKD raises NT-proBNP more than BNP, because the kidney is NT-proBNP’s only exit.
- Obesity lowers BNP more than NT-proBNP, because NPR-C clearance acts on active BNP.
- Sacubitril/valsartan (ARNI, Entresto) makes BNP go UP and become unreliable, neprilysin inhibition blocks BNP breakdown. NT-proBNP is not a neprilysin substrate, so use NT-proBNP to monitor patients on an ARNI.
- Do not switch assays mid-course. Pick BNP or NT-proBNP and trend the same one, the numeric scales are not interchangeable.
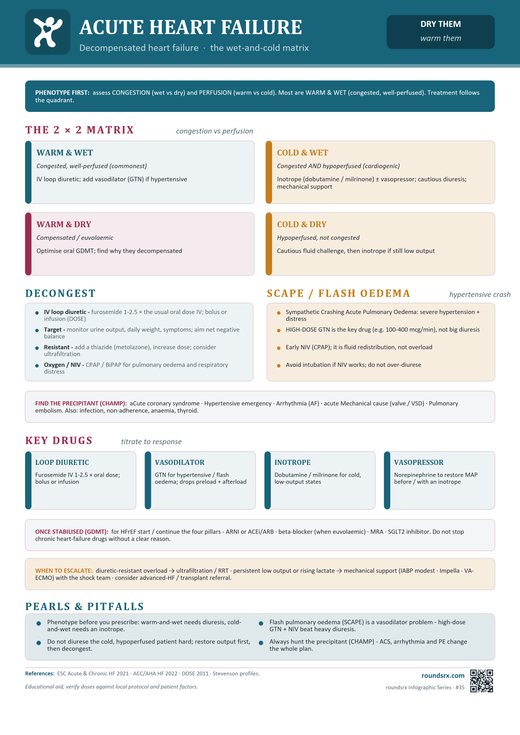 ⤢ Tap to open full size
⤢ Tap to open full size
Text version
🧪 Workup: BNP/NT-proBNP, BMP, troponin, echo, CXR, iron studies. Identify precipitant.
💧 Diurese: IV furosemide 1–2.5× home dose. UOP goal 0.5–1 mL/kg/hr. Add metolazone if resistant.
💊 GDMT: Continue ACEi/ARNI, BB (reduce dose, don’t stop), MRA, SGLT2i. Initiate before discharge.
📈 Monitor: Daily weight, I/Os, BMP (Cr, K⁺), telemetry. Cr bump ≤0.3 acceptable during diuresis.
🏠 Discharge: Stable on PO diuretics ≥24h, at dry weight, GDMT initiated, 7-day follow-up, daily weight education.
STEMI
| Criteria | Definition |
|---|---|
| ST elevation | ≥ 1 mm in ≥ 2 contiguous leads (or ≥ 2 mm in V1–V3 in men, ≥ 1.5 mm in women) |
| Pattern | ECG Findings | Clinical Significance |
|---|---|---|
| New LBBB | New or presumably new LBBB in the setting of ischemic symptoms | Treat as STEMI. Use Sgarbossa criteria if prior LBBB: concordant ST elevation ≥ 1 mm (5 pts), concordant ST depression ≥ 1 mm in V1–V3 (3 pts), discordant ST elevation ≥ 5 mm (2 pts). Score ≥ 3 = MI. Modified Sgarbossa (Smith): ST/S ratio ≥ 0.25 in any lead replaces the 5 mm rule, higher sensitivity. |
| Posterior MI | ST depression V1–V3 with tall R waves ± upright T waves | Reciprocal changes of posterior ST elevation. Get posterior leads (V7–V9): ST elevation ≥ 0.5 mm confirms posterior STEMI. Often occurs with inferior MI (RCA/LCx). Missed in ~75% of cases on standard 12-lead. |
| De Winter T waves | 1–3 mm upsloping ST depression at the J-point with tall, symmetric T waves in precordial leads. No ST elevation. | Proximal LAD occlusion. Present in ~2% of anterior MIs. Static pattern (does not evolve into ST elevation). Activate cath lab immediately. |
| Wellens syndrome | Type A (25%): Biphasic T waves (up-down) in V2–V3. Type B (75%): Deep symmetric T-wave inversions in V2–V3 (± V1–V6) | Critical proximal LAD stenosis. Occurs during pain-free intervals (T waves normalize during active ischemia). Will progress to massive anterior MI without intervention. Do NOT stress test, go to cath lab. |
| Hyperacute T waves | Tall, broad-based, symmetric T waves in a coronary territory. Often taller than the QRS complex. | Earliest sign of acute MI, precedes ST elevation by minutes to hours. Represents subendocardial ischemia with transmural progression. If clinical suspicion is high, serial ECGs q15–30 min or activate cath lab. |
| ST elevation in aVR | Diffuse ST depression in ≥ 6 leads with ST elevation in aVR (± V1) | Left main or proximal LAD occlusion, or severe 3-vessel disease. Very high mortality. Emergent cardiology consultation. Not a classic “STEMI activation” at all centers but requires urgent catheterization. |
| Isolated RV infarction | ST elevation in V4R (> 1 mm) with inferior ST elevation (II, III, aVF). May have ST elevation V1 with depression V2. | Proximal RCA occlusion. Preload-dependent, avoid nitrates, diuretics, morphine. Treat hypotension with IV fluid boluses. Get right-sided leads on all inferior STEMIs. |
| Aslanger pattern | ST elevation in lead III only (not II), with ST depression in any precordial lead, and ST elevation in V1 that does not exceed the ST depression in V6 | Inferior MI with concomitant multi-vessel disease. Subtle pattern, does not meet classic STEMI criteria. Associated with worse outcomes due to multi-vessel involvement. Requires emergent angiography. |
| High Lateral OMI (South African Flag sign) | ST elevation in I and aVL (± V2) with reciprocal ST depression in III and aVF. ST changes may be subtle (< 1 mm) and not meet classic STEMI voltage criteria. | LCx or diagonal branch (D1) occlusion. High lateral territory is poorly represented on standard 12-lead, often missed. The “South African Flag” sign refers to the characteristic ECG morphology resembling the flag’s shape. Low voltage in limb leads makes detection harder. Have a low threshold for cath lab activation with ischemic symptoms + subtle I/aVL changes. |
| ECG Leads | Territory | Artery | Key Complications |
|---|---|---|---|
| V1–V4 | Anterior | LAD | Largest territory. Highest mortality. LV failure, cardiogenic shock, VT/VF, anterior wall aneurysm. |
| II, III, aVF | Inferior | RCA (85%) or LCx (15%) | Bradycardia (AV node from RCA), RV infarct (get right-sided leads V4R). Hypotension -treat with fluids, NOT nitrates. |
| I, aVL, V5–V6 | Lateral | LCx | Often subtle. May be missed. MR from papillary muscle ischemia. |
| V7–V9 | Posterior | PDA (from RCA or LCx) | Missed on standard 12-lead. Always check if ST depression V1–V3. |
| V4R | Right ventricle | Proximal RCA | Avoid nitroglycerin, morphine, diuretics -RV is preload-dependent. Treat hypotension with IV fluids. |
Two large-bore IVs. Continuous cardiac monitoring. 12-lead ECG is the STEMI trigger -ST elevation in ≥2 contiguous leads (or new LBBB with positive Sgarbossa) confirms diagnosis. Supplemental O₂ only if SpO₂ < 90%.
Do NOT swallow whole -chewing provides faster buccal absorption. Continue 81 mg daily lifelong after.
Single phone call. Goal: door-to-balloon < 90 min. Don't wait for troponin to come back -ECG is the trigger. Notify interventionalist, OR team, and transfer team simultaneously.
PCI available within 120 min → Primary PCI (gold standard). Door-to-balloon target < 90 min. Stent the culprit lesion.
PCI not available within 120 min → Fibrinolysis within 30 min of first medical contact. Tenecteplase (weight-based single IV bolus) or alteplase. Transfer for angiography within 3–24h regardless (pharmacoinvasive strategy).
How this differs from NSTEMI: in NSTEMI, you start heparin in the ED right after the diagnosis is confirmed (the patient may not get to cath for hours, so you protect them while they wait). In STEMI, the destination is the cath lab and the wait is short (door-to-balloon < 90 min), so the heparin dose is timed to the procedure -who gives it depends on the reperfusion strategy:
Primary PCI → Heparin is given in the cath lab by the interventionalist, not on the floor. UFH 70–100 units/kg IV bolus, ACT-titrated to 250–300 sec. (Why: ACT-guided dosing in the lab is precise; pre-loading on the floor complicates that titration.) Bivalirudin is an alternative (lower bleeding, slightly higher stent thrombosis).
Fibrinolysis → Heparin is given immediately, as adjunct to the lytic. UFH 60 units/kg IV bolus (max 4000) → 12 units/kg/hr infusion (max 1000/hr). Target aPTT 1.5–2× control. Continue 48h or until revascularization. (Why: there's no cath lab in this scenario, so anticoagulation has to start at the time of lysis to keep the artery open.)
Why STEMI gets P2Y12 upfront, NSTEMI usually defers until cath anatomy is known: In STEMI, the diagnosis is certain (ST elevation = thrombotic occlusion), the destination is certain (cath lab for primary PCI), and CABG-needing anatomy is uncommon (~3–5% of STEMIs, usually a single culprit), so pre-loading lets platelet inhibition reach therapeutic levels by the time of stent deployment. In NSTEMI/UA, ~10–15% turn out to need CABG (3-vessel disease, left main, complex anatomy); pre-loaded ticagrelor or prasugrel force a 5–7 day wait off antiplatelet before surgery, delaying revascularization and increasing in-hospital complications. ACCOAST, 2013 showed upstream prasugrel in NSTEMI did not reduce ischemic events and increased major bleeding, which is why current ACC/AHA guidelines recommend P2Y12 loading at the time of PCI in NSTEMI, not in the ED.
Primary PCI → Ticagrelor 180 mg PO load (preferred) OR prasugrel 60 mg PO load (avoid prior stroke/TIA, age ≥ 75, wt < 60 kg). Clopidogrel 600 mg PO if neither tolerated.
Fibrinolysis → Clopidogrel 300 mg PO load if age < 75; 75 mg PO load if age ≥ 75. CLARITY-TIMI 28, 2005 Ticagrelor and prasugrel are NOT studied with lytics -use clopidogrel.
• Patient can't absorb oral P2Y12 (vomiting, intubated, post-arrest, cardiogenic shock with poor gut perfusion, NPO): use cangrelor IV (preferred -same P2Y12 class, on/off in ~1h) or GP IIb/IIIa as the bridge.
• PCI going badly (large visible thrombus, slow flow / no-reflow, distal embolization, failed reperfusion): add GP IIb/IIIa on top of the oral P2Y12 already given. Interventionalist's call.
• Cath shows CABG-needing anatomy (rare in STEMI -usually a single culprit, but possible): hold further oral P2Y12, bridge with cangrelor or short-acting GP IIb/IIIa until surgery.
• With fibrinolysis: do NOT add GP IIb/IIIa -bleeding risk too high (FINESSE killed this combination).
SL NTG 0.4 mg q5 min × 3, then NTG drip 5–200 mcg/min if pain persists. ⚠️ AVOID in: RV infarct (preload-dependent -check V4R first in inferior MI), SBP < 90, PDE5 inhibitor within 24h (sildenafil) or 48h (tadalafil).
Atorvastatin 80 mg PO (or rosuvastatin 40 mg). Start regardless of LDL -plaque stabilization + anti-inflammatory effects beyond lipid lowering. Lifelong.
Metoprolol tartrate 12.5–25 mg PO q6–12h → titrate to HR 55–65. ⚠️ Hold if: cardiogenic shock, HR < 60, SBP < 100, decompensated HF, cocaine use, severe reactive airway, high-degree AV block. COMMIT-CCS 2, 2005 -early IV BB is harmful in unstable patients; oral BB once stable is the standard.
Lisinopril 2.5–5 mg PO daily (or equivalent). Especially if anterior MI or EF < 40%. Prevents adverse remodeling. Hold if SBP < 100 or AKI.
DAPT: ASA 81 mg + ticagrelor 90 mg BID (or prasugrel 10 mg daily) × 12 months minimum post-ACS DAPT Study, 2014. May shorten to 3–6 months if high bleed risk TWILIGHT, 2019.
High-intensity statin lifelong 4S, 1994
Beta-blocker -continue indefinitely if EF reduced
ACEi/ARB if EF < 40%, HTN, DM, or CKD
Aldosterone antagonist (spironolactone or eplerenone) if EF ≤ 40% + symptomatic HF or DM EPHESUS, 2003
Smoking cessation + cardiac rehab referral
• ASA -give IMMEDIATELY on recognition
• ECG -within 10 minutes
• Cath lab activation -single phone call, don't wait for troponin
• Door-to-balloon < 90 min (primary PCI) or door-to-needle < 30 min (fibrinolysis)
| Drug | Dose | Timing | Notes |
|---|---|---|---|
| Aspirin (antiplatelet) IMMEDIATE | 325 mg chewed (not swallowed) | Immediately on recognition | Chewing provides faster absorption. Continue 81 mg daily indefinitely after. ISIS-2, 1988 |
| Ticagrelor (Brilinta) (antiplatelet) PREFERRED P2Y12 | 180 mg loading → 90 mg BID | At time of PCI (or sooner) | Preferred over clopidogrel PLATO, 2009: reduced CV death + MI + stroke. Reversible binding. Side effects: dyspnea, bradycardia pauses (due to adenosine accumulation -ticagrelor blocks RBC ENT1 reuptake). Do NOT use with > 100 mg ASA. |
| Prasugrel (Effient) (antiplatelet) PREFERRED P2Y12 | 60 mg loading → 10 mg daily | At time of PCI | TRITON-TIMI 38, 2007: superior to clopidogrel. Contraindicated: prior stroke/TIA, age ≥ 75, weight < 60 kg (increased bleeding). |
| Clopidogrel (Plavix) (antiplatelet) 2ND LINE P2Y12 | 600 mg loading → 75 mg daily | At PCI | Use if ticagrelor/prasugrel contraindicated. Prodrug -depends on CYP2C19 metabolism. ~30% of patients are poor metabolizers (consider genetic testing). |
| Heparin (UFH) (anticoagulant) PCI | 70–100 units/kg IV bolus (per cath lab) | At PCI | ACT-guided in cath lab. Bivalirudin is alternative (lower bleeding but higher stent thrombosis). If no PCI planned: enoxaparin 1 mg/kg SC BID is an option ESSENCE, 1997 |
| GP IIb/IIIa inhibitor (tirofiban / Aggrastat, eptifibatide / Integrilin) (antiplatelet) BAILOUT ONLY (bailout = rescue use mid-procedure) | Tirofiban: 25 mcg/kg IV bolus → 0.15 mcg/kg/min infusion. Eptifibatide: 180 mcg/kg IV bolus → 2 mcg/kg/min infusion. | In cath lab if needed -NOT routine, NOT before cath | No longer routine in primary PCI. Reserved for cath-lab bailout: large thrombus burden, slow flow / no-reflow, distal embolization, or as a bridge when P2Y12 absorption is in doubt (vomiting, intubation). FINESSE, 2008 HORIZONS-AMI, 2008 killed routine pre-cath use. Interventionalist's call. Why bailout only? Strongest antiplatelet class (blocks the final common pathway where all aggregation signals converge) but biggest bleeding risk. Modern ticagrelor/prasugrel/cangrelor + bivalirudin + DES now give ~95% of the ischemic benefit with less bleeding -marginal gain no longer worth the bleeding cost. |
| High-intensity statin ALL ACS | Atorvastatin 80 mg or rosuvastatin 40 mg | Within 24h | Start regardless of LDL. Plaque stabilization + anti-inflammatory beyond lipid lowering. Lifelong. PROVE IT-TIMI 22, 2004 4S, 1994 |
| Beta-blocker | Metoprolol 12.5–25 mg PO | Within 24h if stable | Avoid if: cardiogenic shock, HR < 60, SBP < 100, decompensated HF, cocaine use, severe reactive airway. |
| ACEi / ARB | Lisinopril 2.5–5 mg or equivalent | Within 24h | Especially if anterior MI or EF < 40%. Prevents remodeling. Reduce mortality SAVE, 1992. |
| Nitroglycerin (Nitrostat) | 0.4 mg SL q5 min × 3, or drip 5–200 mcg/min | For ongoing chest pain | AVOID in: RV infarct (preload-dependent), SBP < 90, PDE5 inhibitor within 24h (sildenafil) or 48h (tadalafil). Inferior MI → check V4R first. |
| Complication | Timing | Presentation | Diagnosis | Treatment |
|---|---|---|---|---|
| Ventricular free wall rupture | Day 3–7 | Sudden PEA arrest, tamponade | Bedside echo → pericardial effusion | Emergent surgery. Almost always fatal without it. |
| Ventricular septal rupture (VSR) | Day 3–7 | New harsh holosystolic murmur + acute HF | Echo with color Doppler → L-to-R shunt. O₂ step-up on right heart cath. | Surgical repair. IABP/Impella as bridge. Very high mortality. |
| Papillary muscle rupture | Day 2–7 | New holosystolic murmur → acute severe MR → flash pulmonary edema | Echo → flail mitral leaflet, severe MR | Emergent mitral valve surgery. Afterload reduction (nitroprusside, IABP) as bridge. |
| LV aneurysm | Weeks–months | Persistent ST elevation post-MI, HF symptoms, arrhythmias | Echo → dyskinetic/akinetic thin-walled segment | Medical management. Anticoagulation if thrombus. Surgery if refractory arrhythmias. |
| Parameter | Frequency | Target / Action |
|---|---|---|
| Continuous telemetry | Minimum 48 hours post-PCI (longer if EF ≤ 40% or arrhythmias) | Watch for reperfusion arrhythmias (AIVR -usually benign, VT/VF, bradycardia in inferior MI). AIVR is a sign of successful reperfusion -do not treat unless hemodynamically unstable. |
| Serial troponins | q3-6h until peak identified (typically 12-24h post-PCI) | Peak troponin correlates with infarct size. Rising troponin after initial decline → stent thrombosis or reinfarction. |
| ECG | Immediately post-PCI, then daily × 2-3 days | ST resolution > 50% within 60-90 min post-PCI = successful reperfusion. New ST changes → concern for stent thrombosis, re-occlusion. |
| BP and HR | q1h × 4h post-cath, then q4h | SBP > 90 for ACEI/BB initiation. HR 60-80. Hypotension in inferior MI → suspect RV infarct (give fluids, avoid nitroglycerin). |
| Access site | q15min × 1h, then q1h × 4h post-cath | Check for hematoma, bleeding, pseudoaneurysm. Radial: check radial pulse, hand perfusion. Femoral: check distal pulses, retroperitoneal bleed (back pain, Hgb drop). |
| BMP | Daily × 2-3 days, then post-ACEI initiation | Cr (contrast nephropathy peaks 48-72h post-cath). K⁺ > 4.0 and Mg²⁺ > 2.0 for arrhythmia prevention. |
| DAPT compliance | Daily medication reconciliation | ASA 81 mg daily + P2Y12 inhibitor (ticagrelor 90 BID or prasugrel 10 daily). Minimum 12 months post-DES. Premature DAPT discontinuation = stent thrombosis risk. |
| Echocardiogram | Within 24-48h post-PCI | EF, wall motion, mechanical complications (VSD -new murmur + hemodynamic collapse; papillary muscle rupture -acute MR). Repeat at 6-12 weeks if EF ≤ 40%. |
| Test | Rationale | Key Values |
|---|---|---|
| 12-lead ECG | Diagnose STEMI. Identify culprit territory. Repeat q15 min if evolving or diagnostic uncertainty. | ≥ 1 mm ST elevation in 2 contiguous leads (≥ 2 mm in V1-V3 for men > 40). New LBBB with ischemic symptoms. Right-sided leads (V4R) for inferior STEMI → RV involvement. |
| Serial troponins | Confirm myocardial injury and trend infarct size. Do NOT wait for troponin to activate cath lab in STEMI. | Draw at presentation, then q3-6h × 3. Peak troponin correlates with infarct size. High-sensitivity troponin (hs-cTnI or hs-cTnT). |
| CBC | Baseline Hgb (bleeding risk with anticoagulation/DAPT), platelets (for P2Y12 inhibitor). | Hgb < 10 = higher bleeding risk with aggressive antithrombotics. Plt < 100K = relative contraindication to DAPT. |
| BMP | Cr (contrast nephropathy risk, ACEI dosing), K⁺ (arrhythmia risk), glucose (stress hyperglycemia). | K⁺ > 4.0 and Mg²⁺ > 2.0 to minimize arrhythmia risk. Cr for contrast load planning. |
| Coagulation (PT/INR, aPTT) | Baseline before heparin. Identify existing anticoagulation. | Needed before heparin bolus in cath lab. |
| Lipid panel | Draw within 24h (acute-phase changes lower LDL after 24-48h). | Start high-intensity statin regardless of LDL. LDL target < 70 (some guidelines < 55). |
| BNP / NT-proBNP | Prognostication. Elevated BNP = higher risk of HF and mortality post-MI. | Guides post-MI HF risk stratification. |
| Echocardiogram | Assess EF, wall motion abnormalities (correlate with culprit vessel), mechanical complications (VSD, papillary muscle rupture, free wall rupture). | Obtain within 24-48h post-PCI. EF ≤ 40% → ACEI/ARB + aldosterone antagonist. New MR → papillary muscle dysfunction. |
| Type and screen | In case of bleeding complication or need for emergent surgery. | Standard pre-procedural lab. |
| Phase | Time | Action | Rationale / Pearl |
|---|---|---|---|
| ED Arrival | T+0 min | 12-lead ECG within 10 minutes | ECG shows ST elevation V1-V4 with reciprocal ST depression in II, III, aVF. This is an anterior STEMI -LAD territory. Activate cath lab immediately. |
| Immediate Meds | T+5 min | ASA 325 mg (chewed) + ticagrelor 180 mg PO + heparin 60 U/kg bolus + atorvastatin 80 mg | Chew ASA for rapid absorption. Load P2Y12 inhibitor before cath. Heparin for anticoagulation during PCI. Statin started day 1 regardless of lipid panel. |
| Cath Lab | T+48 min | PCI to LAD: 99% proximal occlusion. Drug-eluting stent (DES) placed. TIMI 3 flow restored. | Door-to-balloon = 48 min (goal < 90 min). Complete occlusion confirmed -this is why ECG, not troponin, drives the decision. Troponin was still negative at arrival. |
| Troponin #1 | T+0 (arrival) | hs-cTnI: 45 ng/L (normal < 26) | Only mildly elevated at presentation -do not wait for troponin to confirm STEMI. ECG is the decision tool. Early troponin may be falsely reassuring in early presenters. |
| Troponin #2 | T+3h | hs-cTnI: 12,400 ng/L (> 250× ULN). Rising rapidly. | Large delta = large infarct. Rapid rise-and-fall pattern typical of reperfused STEMI. Expected to peak 12-24h post-onset. |
| Troponin #3 | T+6h | hs-cTnI: 38,600 ng/L. Still rising. | Continue trending q6h. The magnitude of peak predicts LV dysfunction severity and 30-day mortality. > 10,000 ng/L in anterior STEMI = high risk for EF < 40%. |
| Troponin #4 (peak) | T+12h | hs-cTnI: 85,000 ng/L (peak). Begins declining thereafter. | Peak troponin reached ~12h post-symptom onset. Large anterior MI confirmed. Correlates with TTE findings. Subsequent decline = no re-occlusion. Any secondary rise → suspect stent thrombosis. |
| CCU Day 1 | T+3h | Chest pain resolved. Troponin peaks at 85 ng/mL. TTE: EF 40%, anterior wall hypokinesis. | Peak troponin correlates with infarct size. EF 40% -will need ACEi/ARB and assess for ICD at 40 days. Start metoprolol 25 mg BID if hemodynamically stable. |
| Day 2 | T+24h | Troponin trending down: 42,000 → 18,000 ng/L. Start lisinopril 2.5 mg, uptitrate metoprolol. Cardiac rehab consult. Smoking cessation counseling. | Declining troponin = reassuring (no re-occlusion). ACEi started for EF ≤ 40% (reduces remodeling and mortality). BB reduces arrhythmia risk. Early rehab referral improves adherence and outcomes. |
| Discharge (Day 3) | ASA 81 mg + ticagrelor 90 BID (DAPT × 12 months). Metoprolol succinate 50 mg daily. Lisinopril 5 mg. Atorvastatin 80 mg. Cardiac rehab. Follow-up in 1 week. | Ensure all 4 pillars prescribed before discharge. LDL goal < 70 (or < 55 per ESC). Repeat TTE in 6-12 weeks. Discuss ICD if EF still ≤ 35% at 40 days. |
| Phase | Time | Action | Rationale / Pearl |
|---|---|---|---|
| ED Arrival | T+0 | ECG: ST elevation II, III, aVF. Reciprocal depression I, aVL. | Inferior STEMI -RCA territory (85%). Immediately get right-sided leads (V4R). V4R shows ST elevation ≥ 1mm -confirms RV infarct. |
| Critical Decision | T+3 min | NO nitroglycerin. NO morphine. Start 500 mL NS bolus. | RV infarct = preload dependent. Nitrates and morphine drop preload → cardiovascular collapse. Fluids first. If still hypotensive after 1-2L, start dobutamine (not norepinephrine -need inotropy, not vasoconstriction). |
| Meds | T+8 min | ASA 325 + clopidogrel 600 (not ticagrelor -patient is bradycardic). Heparin. Atropine 0.5 mg IV for symptomatic bradycardia. | Ticagrelor can worsen bradycardia (PLATO showed more bradycardic pauses). Clopidogrel is safer here. Atropine for vagally-mediated bradycardia (common in inferior MI due to RCA supplying AV node). |
| Cath Lab | T+62 min | PCI to RCA: 100% mid-vessel occlusion. DES placed. TIMI 3 flow. BP improves to 106/68. | RCA reperfusion often dramatically improves hemodynamics. Bradycardia may resolve as AV node perfusion returns. If persistent complete heart block → temporary pacer. |
| Troponin #1 | T+0 (arrival) | hs-cTnI: 180 ng/L (elevated > 26) | Elevated at presentation -1 hour of symptoms means troponin is already rising. In inferior STEMI, absolute values tend to be lower than anterior (smaller territory). Still -do NOT wait for troponin result. |
| Troponin #2 | T+3h | hs-cTnI: 5,800 ng/L. Rising. | Moderate elevation consistent with RCA territory (supplies ~25-30% of LV). Compare: LAD occlusion often produces troponins > 50,000. |
| Troponin #3 (peak) | T+8h | hs-cTnI: 14,200 ng/L (peak). | Earlier peak than anterior STEMI (smaller territory = faster washout post-reperfusion). Declining troponin + improving hemodynamics = successful reperfusion. Any secondary rise → re-occlusion or stent thrombosis. |
| CCU Day 1 | T+6h | Sinus rhythm restored, HR 68. BP 110/72 on 150 mL/hr NS. TTE: EF 50%, inferior hypokinesis, RV dilated but improving. Troponin trending down. | RV function often recovers within days-weeks (RV is more resilient than LV). Avoid diuretics -patient needs volume. Hold ACEi until hemodynamically stable. |
| Day 2-3 | Troponin 3,400 → 890 ng/L (steadily declining). Wean fluids. Start low-dose metoprolol if HR tolerates. Start lisinopril 2.5 mg cautiously (monitor BP). | RV infarct patients are exquisitely sensitive to volume depletion AND afterload reduction. Titrate meds slowly. If EF preserved, ACEi is less urgent but still beneficial. | |
| Discharge (Day 4) | ASA 81 + clopidogrel 75 × 12 months. Metoprolol succinate 25 mg. Lisinopril 2.5 mg. Atorvastatin 80 mg. Strict diabetes management (A1c target < 7). | Key teaching: Always check V4R in inferior STEMI. RV infarct changes your entire management -no nitrates, aggressive fluids, be cautious with preload-reducing drugs. |
| Phase | Time | Action | Rationale / Pearl |
|---|---|---|---|
| ED Arrival | T+0 | ECG: ST elevation V1-V6, I, aVL (massive anterolateral). Chest X-ray: bilateral pulmonary edema. | Extensive anterior STEMI with Killip Class IV (cardiogenic shock). This is the highest-risk presentation -mortality 40-50% even with PCI. Do NOT delay cath for stabilization. |
| Immediate | T+5 min | ASA 325 + clopidogrel 600 (avoid ticagrelor in shock -absorption unreliable). Heparin. Activate cath lab. Place arterial line. Start norepinephrine 0.1 mcg/kg/min. | Cardiogenic shock = primary PCI regardless of time from onset. Norepinephrine is first-line vasopressor in cardiogenic shock (SOAP II trial). Avoid dopamine (more arrhythmias). Load P2Y12 via NG if vomiting. |
| Pre-Cath | T+15 min | Intubated for respiratory failure and impaired consciousness. PA catheter placed: CI 1.6, PCWP 28, SVR 1800. | PA catheter confirms cardiogenic shock: low CI (< 2.2), high PCWP (> 18), high SVR. BiPAP is an alternative if patient is alert, but this patient is deteriorating. |
| Cath Lab | T+55 min | PCI to LAD: 100% proximal occlusion. DES placed. TIMI 2 flow (incomplete reperfusion). Intra-aortic balloon pump (IABP) placed. | TIMI 2 flow (partial) has worse prognosis than TIMI 3 (complete). Mechanical circulatory support (IABP or Impella) considered for refractory shock. IABP-SHOCK II showed no mortality benefit for IABP, but still used as bridge. |
| Troponin #1 | T+0 (arrival) | hs-cTnI: 28,400 ng/L (massively elevated) | Already very high at presentation -6 hours of unreperfused ischemia. In cardiogenic shock, troponin may be falsely lower due to decreased cardiac output (poor washout). Once reperfused, expect a secondary surge. |
| Troponin #2 | T+3h post-PCI | hs-cTnI: 96,000 ng/L. Massive surge post-reperfusion. | Reperfusion washout phenomenon: troponin spikes after PCI as necrotic myocardium is reperfused and cellular contents flood the circulation. Higher post-PCI spike = more necrosis, not a new event. |
| Troponin #3 | T+12h | hs-cTnI: 142,000 ng/L (peak). | Late presenters (6h+) have the highest peak troponins. TIMI 2 flow means incomplete washout -troponin may plateau longer. This level predicts severe LV dysfunction and high 30-day mortality. |
| Troponin #4 | T+24h | hs-cTnI: 98,000 ng/L. Beginning to decline. | Slow decline expected with TIMI 2 flow. If troponin re-rises → stent thrombosis, extension of infarct, or type 2 MI from shock. Recheck ECG immediately. |
| CCU Day 1-2 | Persistent shock on norepi + dobutamine. TTE: EF 15%, diffuse anterior akinesis. Lactate trending down from 6.8 to 3.1. Cr rising (1.1 → 2.3). Troponin 98,000 → 54,000 ng/L. | Multiorgan dysfunction from prolonged cardiogenic shock. Add milrinone if dobutamine insufficient. Avoid aggressive diuresis -cardiorenal syndrome. Consider Impella if failing IABP. | |
| Day 3-5 | Slowly weaning vasopressors. Extubated Day 4. Watch for mechanical complications (VSD, papillary rupture -classically Day 3-7). | Day 3-7 is the danger zone for mechanical complications. New murmur + hemodynamic collapse = STAT TTE. Free wall rupture presents as sudden PEA arrest with tamponade. | |
| Day 7-10 | Off pressors. EF 20% on repeat TTE. Start captopril 6.25 mg TID (short-acting, easy to titrate). Careful diuresis with IV furosemide. | Use short-acting ACEi (captopril) initially -if BP drops, it wears off in hours. Sacubitril/valsartan NOT in acute phase (< 36h post-MI). Start after stabilization. | |
| Discharge (Day 14) | ASA 81 + clopidogrel 75 × 12 months. Carvedilol 3.125 BID. Captopril 12.5 TID (switch to sacubitril/valsartan outpatient). Atorvastatin 80. Eplerenone 25 mg. Furosemide PRN. LifeVest (wearable defibrillator) until 40-day EF reassessment for ICD. | EF 20% → high SCD risk. LifeVest bridges to 40-day reassessment (don't implant ICD immediately -EF may recover). If EF still ≤ 35% at 40 days → ICD. Refer for advanced HF evaluation if no recovery. |
| Phase | Time | Action | Rationale / Pearl |
|---|---|---|---|
| ED Arrival | T+0 | ECG: No ST elevation. But -ST depression V1-V3, tall R waves in V1-V2 (R/S ratio > 1). Subtle but there. | This IS a STEMI. ST depression V1-V3 with tall R waves = posterior MI (mirror image). The standard 12-lead has NO posterior-facing leads. This is the most commonly missed STEMI. |
| Key Move | T+5 min | Posterior leads V7-V9. V7-V9 show ST elevation ≥ 0.5 mm. | Posterior STEMI confirmed. This is a STEMI equivalent -activate cath lab immediately. LCx or PDA (from RCA) territory. Any ST elevation ≥ 0.5 mm in posterior leads is diagnostic. |
| Meds | T+8 min | ASA 325 + ticagrelor 180 + heparin + atorvastatin 80. Cath lab activated. | Standard STEMI protocol. Do NOT wait for troponin to confirm. The posterior leads are your proof. |
| Cath Lab | T+72 min | PCI to LCx: 100% mid-vessel occlusion. DES placed. TIMI 3 flow. | LCx occlusion confirmed. Door-to-balloon 72 min. Without posterior leads, this patient would have been admitted as "NSTEMI" and waited hours-days for cath. |
| Troponin #1 | T+0 (arrival) | hs-cTnI: 620 ng/L (elevated) | 2 hours of symptoms -troponin already elevated. In posterior STEMI, the ECG may look "normal" but the troponin confirms myocardial injury. However the posterior leads, NOT the troponin, drove the cath lab activation. |
| Troponin #2 | T+3h | hs-cTnI: 4,200 ng/L. Rising. | LCx territory is smaller than LAD -expect moderate (not massive) troponin elevation. Peak troponins in LCx STEMI are typically 5,000-25,000 ng/L range. |
| Troponin #3 (peak) | T+8h | hs-cTnI: 9,800 ng/L (peak). | Moderate peak -consistent with smaller infarct territory and good TIMI 3 reperfusion. Early reperfusion limits infarct size. Declining troponin + preserved EF = excellent prognosis. |
| CCU Day 1 | Pain free. Troponin trending down: 6,100 ng/L. TTE: EF 55%, mild posterior/lateral hypokinesis. Mild MR (papillary muscle ischemia). | Good EF because LCx territory is smaller than LAD. Mild MR from posterior papillary muscle -monitor with serial TTE. Usually improves with reperfusion. | |
| Discharge (Day 2) | ASA 81 + ticagrelor 90 BID × 12 months. Metoprolol succinate 25 mg. Atorvastatin 80. Cardiac rehab. No ACEi needed (EF preserved). | Key teaching: "Normal" ECG + ACS symptoms → get posterior leads. ST depression V1-V3 is never normal in ACS. This diagnosis is made by the physician who thinks of it, not by the ECG machine's algorithm. |
| Phase | Time | Action | Rationale / Pearl |
|---|---|---|---|
| ED Arrival | T+0 | ECG: ST elevation V1-V4. STEMI criteria met. But -is this true coronary occlusion or cocaine-induced vasospasm? | Doesn't matter initially -treat as STEMI. Activate cath lab. Can distinguish at angiography. 6% of cocaine chest pain has real MI. |
| Critical Meds | T+3 min | ASA 325 mg. Benzodiazepine (diazepam 5-10 mg IV). Nitroglycerin 0.4 mg SL. NO BETA-BLOCKERS. | Beta-blockers are CONTRAINDICATED in cocaine MI -causes unopposed alpha stimulation → worsens coronary vasospasm and hypertension. Benzos reduce sympathetic drive. Nitro treats vasospasm. If nitro + benzo resolve ST elevation → likely vasospasm, not thrombotic occlusion. |
| Response | T+15 min | After diazepam + nitro: ST elevation persists. Pain ongoing. → Proceed to cath lab. | If ST changes resolve with benzos + nitro → observe, serial ECGs, troponins. If ST changes persist → angiography. This patient has persistent ST elevation → real occlusion until proven otherwise. |
| Cath Lab | T+58 min | PCI to LAD: Thrombus with 90% stenosis in a young vessel. Aspiration thrombectomy + DES. TIMI 3 flow. | Cocaine causes MI via: (1) coronary vasospasm, (2) accelerated atherosclerosis, (3) increased platelet aggregation, (4) increased myocardial oxygen demand. This patient had both thrombus AND underlying disease. |
| Troponin #1 | T+0 (arrival) | hs-cTnI: 52 ng/L (mildly elevated) | Only mildly elevated -cocaine was used 2h ago, but coronary occlusion may be more recent. Key point: if ST elevation resolves with benzos + nitro AND troponin is normal → vasospasm. If troponin rises → true infarction regardless of vasospasm resolution. |
| Troponin #2 | T+3h | hs-cTnI: 6,800 ng/L. Significant rise confirms infarction. | Rising troponin confirms true MI -not just vasospasm. Cocaine-induced MI can have both components (spasm + thrombus). The delta (52 → 6,800) confirms acute necrosis. |
| Troponin #3 (peak) | T+8h | hs-cTnI: 18,400 ng/L (peak). | Moderate peak -aspiration thrombectomy + early reperfusion limited infarct size. Young vessels with less collateral disease may paradoxically have larger infarcts (no collateral protection). Monitor for decline. |
| CCU Day 1 | Symptom free. Troponin declining: 11,200 ng/L. TTE: EF 50%. Start amlodipine 5 mg (vasodilator, safe in cocaine). Still no beta-blocker. | CCB (amlodipine or diltiazem) is safe and treats both vasospasm and hypertension. Can consider non-selective BB (carvedilol) only after cocaine fully cleared (24-48h) and only if clear cardiac indication. | |
| Discharge (Day 3) | ASA 81 + ticagrelor 90 BID × 12 months. Amlodipine 5 mg. Atorvastatin 80. Substance abuse counseling. Psychiatry referral. Social work. | Discharge prescription without addressing cocaine use = guaranteed readmission. Substance abuse consult is as important as the stent. Document the conversation. Arrange follow-up. |
🧪 Workup: Focused labs + imaging → see Workup tab
⚡ Treat: Evidence-based algorithm → see Management tab
💊 Drugs: Key medications with dosing → see Medications tab
📈 Monitor: Telemetry ≥48h, serial troponins, ECG post-PCI, access site checks, BMP daily
📣 Present: One-liner + key points → see Rounds tab
| Parameter | Frequency | Target / Action |
|---|---|---|
| Continuous telemetry | Minimum 48h post-PCI (longer if EF ≤40%) | Reperfusion arrhythmias: AIVR (benign = successful reperfusion), VT/VF, bradycardia in inferior MI. |
| Serial troponins | q3–6h until peak (typically 12–24h post-PCI) | Peak troponin correlates with infarct size. Re-elevation after decline → stent thrombosis or reinfarction. |
| ECG | Immediately post-PCI, then daily ×2–3 days | ST resolution >50% within 60–90 min = successful reperfusion. New ST changes → stent thrombosis. |
| Access site | q15min ×1h, then q1h ×4h post-cath | Hematoma, bleeding, pseudoaneurysm. Radial: pulse + hand perfusion. Femoral: distal pulses, retroperitoneal bleed (back pain, Hgb drop). |
| BP / HR | q1h ×4h post-cath, then q4h | SBP >90 for ACEi/BB initiation. Hypotension in inferior MI → suspect RV infarct (fluids, avoid NTG). |
| BMP | Daily ×2–3 days + post-ACEi initiation | Cr (contrast nephropathy peaks 48–72h). K⁺ >4.0, Mg²⁺ >2.0 for arrhythmia prevention. |
| Echo | Within 24–48h post-PCI | EF, wall motion, mechanical complications (VSD, papillary muscle rupture, free wall rupture at day 3–7). Repeat at 6–12 wk if EF ≤40%. |
| DAPT compliance | Daily medication reconciliation | ASA 81 mg + P2Y12 inhibitor (ticagrelor 90 BID or prasugrel 10 daily). Minimum 12 months post-DES. Premature stop = stent thrombosis. |
- ST elevation ≥ 1mm in ≥ 2 contiguous leads (≥ 2mm in V1-V3)
- New LBBB with ischemic symptoms
- Posterior MI: ST depression V1-V3 → get V7-V9
- Troponin may be normal initially -ECG is the decision tool
- ASA 325 mg chewed + P2Y12 load (ticagrelor 180 mg)
- Heparin bolus + drip
- Activate cath lab → PCI
- Atorvastatin 80 mg
- Morphine only if refractory pain (may reduce P2Y12 absorption)
- II, III, aVF = Inferior (RCA)
- V1-V4 = Anterior (LAD)
- I, aVL, V5-V6 = Lateral (LCx)
- V3R, V4R = Right ventricle (check if inferior STEMI)
- Delaying PCI for "stabilization"
- Missing posterior/RV STEMI
- Nitro in RV infarct (preload dependent)
- No DAPT × 12 months post-PCI
NSTEMI / Unstable Angina
| Feature | NSTEMI | Unstable Angina |
|---|---|---|
| Troponin | Elevated (rise and/or fall) | Normal |
| ECG | ST depression, T-wave inversions, or nonspecific (NO ST elevation) | Same -may be normal |
| Pathology | Partial/intermittent occlusion with myocardial necrosis | Partial/intermittent occlusion without necrosis |
| Management | Same initial management. NSTEMI → higher risk → earlier invasive strategy. | Risk-stratify. May be managed conservatively if low-risk. |
| Component | 0 Points | 1 Point | 2 Points |
|---|---|---|---|
| H -History | Non-suspicious | Moderately suspicious | Highly suspicious |
| E -ECG | Normal | Non-specific repolarization changes | Significant ST deviation |
| A -Age | < 45 | 45–64 | ≥ 65 |
| R -Risk factors | None | 1–2 factors | ≥ 3 factors or known CAD |
| T -Troponin | Normal | 1–3× ULN | > 3× ULN |
| Score | Risk | Action |
|---|---|---|
| 0–3 | Low (< 2% MACE at 6 weeks) | Consider early discharge with outpatient follow-up. Stress test if needed. |
| 4–6 | Intermediate | Admit, observe, serial troponins. Consider angiography. |
| 7–10 | High (> 50% MACE) | Early invasive strategy -angiography within 24h. |
| Variable | 1 Point If Present |
|---|---|
| Age ≥ 65 | Yes / No |
| ≥ 3 CAD risk factors | HTN, DM, dyslipidemia, smoking, family hx of premature CAD |
| Known CAD (stenosis ≥ 50%) | Prior coronary stenosis ≥ 50% on cath |
| ASA use in past 7 days | Suggests breakthrough event despite aspirin |
| ≥ 2 anginal episodes in 24h | Recurrent ischemia = higher risk |
| ST deviation ≥ 0.5 mm | ST depression or transient ST elevation on ECG |
| Elevated cardiac biomarkers | Troponin or CK-MB above upper limit of normal |
| TIMI Score | 14-Day Event Rate | Risk Level | Action |
|---|---|---|---|
| 0–2 | 4.7% | Low | Conservative management. Consider early discharge if HEART score also low. |
| 3–4 | 13.2% | Intermediate | Admit. Consider angiography within 24–72h. |
| 5–7 | 40.9% | High | Early invasive strategy -cath within 24h. Consider ICU-level monitoring. |
| Variable | Details |
|---|---|
| Age | Continuous -higher age = more points (e.g., 60 yo = ~58 pts, 80 yo = ~91 pts) |
| Heart rate | Higher HR = more points (e.g., HR 100 = ~15 pts, HR 150 = ~42 pts) |
| Systolic BP | Inverse -lower SBP = more points (SBP 80 = ~63 pts, SBP 160 = ~12 pts) |
| Creatinine | Higher Cr = more points (renal dysfunction worsens prognosis) |
| Killip class | I (no HF) = 0 pts → IV (cardiogenic shock) = ~64 pts |
| Cardiac arrest at presentation | Yes = +43 pts |
| ST-segment deviation | Yes = +30 pts |
| Elevated cardiac enzymes | Yes = +15 pts |
| GRACE Score | In-Hospital Mortality | Risk Level | Action |
|---|---|---|---|
| ≤ 108 | < 1% | Low | Conservative strategy. Stress test before discharge. |
| 109–140 | 1–3% | Intermediate | Consider angiography within 24–72h based on other features. |
| > 140 | > 3% | High | Early invasive strategy -cath within 24h. |
I -No heart failure signs
II -Rales, S3, elevated JVP (mild HF)
III -Acute pulmonary edema
IV -Cardiogenic shock (SBP < 90, end-organ hypoperfusion)
12-lead ECG within 10 minutes. Establish 2 large-bore IVs. Continuous cardiac monitoring. Supplemental O₂ only if SpO₂ < 90%.
Do NOT swallow whole -chewing provides faster buccal absorption. Continue 81 mg daily lifelong after.
SL NTG 0.4 mg q5min × 3, then NTG drip 5–200 mcg/min if pain persists. ⚠️ Contraindications: SBP < 90, RV infarct (check right-sided ECG), PDE5 inhibitor within 24–48h.
Give to all NSTE-ACS unless contraindicated (active bleeding, recent ICH, known HIT). Risk scores guide cath timing, NOT the decision to anticoagulate.
UFH drip: 60 U/kg bolus (max 4,000) → 12 U/kg/hr (max 1,000). Target aPTT 1.5–2.5× control.
OR Enoxaparin: 1 mg/kg SC BID (if no PCI planned within 24h, CrCl > 30) ESSENCE, 1997
⚠️ Do NOT switch between heparin types (increases bleeding risk).
TIMI score Quick bedside -7 yes/no questions, 1 point each. Predicts 14-day death/MI/urgent revasc. Fast to calculate at the bedside; higher score = more benefit from early invasive strategy. TIMI 11B, 1998
HEART score ED disposition -best for deciding who goes home vs who gets admitted. 0–3 = low risk (< 2% MACE), safe for early discharge with outpatient follow-up.
GRACE score Most accurate mortality prediction -in-hospital and 6-month mortality. Drives invasive strategy timing: GRACE > 140 = cath within 24h. Use for all admitted NSTEMI patients.
Serial troponins q3–6h -watch for rise and/or fall pattern.
GRACE > 140 or high-risk features → Early invasive (cath within 24h)
GRACE 109–140 (intermediate risk) → Delayed invasive (cath within 24–72h)
GRACE ≤ 108, negative troponins, no high-risk features → Conservative. Stress test if needed.
| Strategy | Who | Timing | Notes |
|---|---|---|---|
| Immediate invasive (< 2h) | Refractory angina, hemodynamic instability, VT/VF, acute HF | Emergent cath | This is essentially a STEMI-equivalent presentation without ST elevation. |
| Early invasive (≤ 24h) | GRACE > 140, rising troponin, new ST changes, dynamic ECG changes | Cath within 24h | TIMACS, 2009: early (< 24h) vs delayed (> 36h) → reduced refractory ischemia in high-risk patients (GRACE > 140). |
| Delayed invasive (24–72h) | GRACE 109–140, intermediate risk (e.g., diabetes, EF < 40%, post-MI angina, prior PCI/CABG, GFR < 60) | Cath within 72h | Acceptable for stable patients. Load P2Y12 when anatomy known (cath lab). |
| Conservative / ischemia-guided | GRACE ≤ 108, no recurrent symptoms, negative serial troponins, no high-risk features | Stress test if needed | Medical management. Cath only if stress test positive or recurrent symptoms. |
Going to cath → Load in the cath lab AFTER coronary anatomy is known (preserves CABG option -ticagrelor/clopidogrel delay surgery 5–7 days).
Conservative strategy → Load upfront (ticagrelor 180 mg or clopidogrel 600 mg).
Preferred: Ticagrelor 90 mg BID (reversible, faster onset, no CYP2C19 resistance). Prasugrel if going to PCI and no contraindications (prior stroke/TIA, age ≥75, wt <60 kg).
| Agent | Loading | Maintenance | Mechanism | Notes |
|---|---|---|---|---|
| Ticagrelor (Brilinta) PREFERRED | 180 mg PO | 90 mg BID | Reversible | Faster onset, no CYP2C19 issue. Side effects: dyspnea, bradycardia (adenosine accumulation -blocks RBC ENT1 reuptake). Do NOT use with ASA > 100 mg. |
| Prasugrel (Effient) | 60 mg PO | 10 mg daily | Irreversible | Only after anatomy known (PCI confirmed). Contraindicated: prior stroke/TIA. Avoid: age ≥ 75, wt < 60 kg. |
| Clopidogrel (Plavix) 2ND LINE | 600 mg PO | 75 mg daily | Irreversible (prodrug) | Use if ticagrelor/prasugrel contraindicated. ~30% of patients are CYP2C19 poor metabolizers (consider genetic testing). |
| Cangrelor (Kengreal) IV OPTION | 30 mcg/kg IV bolus | 4 mcg/kg/min infusion | Reversible (IV) | For cath lab if patient can't take PO or needs immediate platelet inhibition. Bridge until oral P2Y12 onset. |
Bailout role only: high thrombus burden, slow flow / no-reflow, or bridge when P2Y12 absorption is in doubt (vomiting, intubation). EARLY ACS, 2009 showed pre-cath use adds bleeding without benefit. Why bailout only? Strongest antiplatelet class (blocks final common pathway) but biggest bleeding risk -modern P2Y12 + bivalirudin + DES deliver ~95% of the ischemic benefit with less bleeding.
• Stable CAD: PCI does NOT beat optimal medical therapy on hard outcomes COURAGE, 2007
• Multivessel / left-main: CABG preferred for complex anatomy SYNTAX, 2009
• Diabetics with multivessel CAD: CABG beats PCI FREEDOM, 2012
Atorvastatin 80 mg PO (or rosuvastatin 40 mg). Start regardless of LDL -plaque stabilization + anti-inflammatory effects beyond lipid lowering. Lifelong.
Metoprolol tartrate 12.5–25 mg PO q6–12h → titrate to HR 55–65. ⚠️ Hold if: SBP < 100, HR < 60, active HF/pulmonary edema, cocaine use, high-degree AV block. Defer until after the invasive/conservative decision and hemodynamic status is clear -BB is not emergent.
DAPT: ASA 81 mg + ticagrelor 90 mg BID × 12 months (minimum 6 months if high bleed risk) PLATO, 2009
High-intensity statin lifelong 4S, 1994
Beta-blocker (continue indefinitely if EF reduced)
ACEi/ARB if EF < 40%, HTN, DM, or CKD
Smoking cessation + cardiac rehab referral
• Aspirin -give IMMEDIATELY on recognition
• ECG -within 10 minutes
• Heparin -start as soon as NSTEMI/UA diagnosis confirmed (STEMI primary PCI = give in cath lab; STEMI lytic = give as adjunct in the ED)
• Cath -within 2h if hemodynamically unstable (treat like STEMI)
Management: Aspirin 325 mg chewed immediately, heparin drip (60 U/kg bolus → 12 U/kg/hr), atorvastatin 80 mg, metoprolol tartrate 12.5 mg PO BID. GRACE score 148, early invasive strategy, cath within 24 hours. P2Y12 inhibitor loading deferred until coronary anatomy known in the cath lab to preserve CABG option. NTG SL PRN for recurrent chest pain.
Management: This is Type 2 MI (demand ischemia), tachycardia and hypoxemia from pneumonia caused supply-demand mismatch, not plaque rupture. Treat the underlying pneumonia, not with cath. Avoid aggressive anticoagulation or invasive strategy. Start atorvastatin 80 mg for secondary prevention. Cardiology consult for outpatient stress test after pneumonia resolves. Serial troponins to confirm downtrend.
Management: This is NSTEMI with cardiogenic shock, treat as STEMI equivalent. Emergent cath (< 2 hours). Start norepinephrine for hemodynamic support (avoid dobutamine alone if SBP < 90). Consider IABP or Impella for mechanical circulatory support. Cath reveals multivessel disease, culprit PCI now, then heart team discussion for staged PCI vs CABG for remaining lesions. Hold beta-blocker until hemodynamically stable. ICU admission mandatory.
| Parameter | Frequency | Target / Action |
|---|---|---|
| Continuous telemetry | Duration of hospitalization (minimum 24-48h) | Monitor for VT/VF, new AF, bradycardia, ST changes. Ischemic ST changes on telemetry → repeat 12-lead ECG immediately. |
| Serial troponins | At presentation, 3h, 6h (until peak identified) | Rising pattern confirms NSTEMI. Plateau or decline = peak identified. Re-elevation after decline → reinfarction or stent thrombosis. |
| Chest pain assessment | q4h nursing assessment + PRN | Recurrent chest pain → repeat ECG, consider NTG, notify cardiology. Refractory pain = indication for urgent cath. |
| BP | q4h (q1h if on NTG drip or hemodynamically unstable) | SBP ≥ 90 for beta-blocker and ACEi initiation. Hold NTG if SBP < 90. Target HR 60-70 with beta-blocker. |
| HR | q4h; continuous on telemetry | Tachycardia > 100 → pain? anxiety? HF? bleeding? Bradycardia < 50 → hold BB, check for conduction disease. |
| aPTT (if on heparin drip) | q6h until therapeutic, then q12h | Goal aPTT 60-80 seconds (1.5-2.5× control). Adjust per institutional heparin nomogram. |
| BMP | Daily; post-cath (contrast nephropathy) | K⁺ > 4.0, Mg²⁺ > 2.0. Cr at 24 and 48h post-contrast. Cr rise > 0.5 = contrast nephropathy. |
| Hgb / Hct | Daily; more frequently if on anticoagulation or post-cath | Hgb drop > 2 without overt bleeding → access site bleed? retroperitoneal hemorrhage? GI bleed? |
| Test | Rationale | Key Values |
|---|---|---|
| Serial troponins | Diagnose NSTEMI (rising/falling pattern). Draw at presentation, 3h, and 6h. Unstable angina = negative troponins with ischemic symptoms. | hs-cTnI or hs-cTnT: rising delta > 20% from baseline = acute injury. Peak troponin correlates with infarct size and prognosis. |
| 12-lead ECG | ST depressions, T-wave inversions, or dynamic changes. Repeat with any symptom recurrence. | ST depression ≥ 0.5 mm in 2+ contiguous leads. New TWI ≥ 1 mm. Normal ECG does NOT exclude NSTEMI. Wellens' pattern (deep symmetric TWI in V2-V3) = critical LAD stenosis. LCx occlusion is often electrically silent -standard 12-lead has no posterior-facing leads, so isolated posterior/lateral wall ischemia may show only subtle ST depression in V1–V3 or no changes at all. If clinical suspicion is high despite a normal ECG, get posterior leads (V7–V9) and maintain a low threshold for serial ECGs and troponins. |
| HEART score | Risk stratification for chest pain. Guides disposition (discharge vs admit vs cath). | 0-3 = low risk (1.7% MACE, consider discharge). 4-6 = moderate (12% MACE, admit). 7-10 = high (65% MACE, early invasive). |
| TIMI risk score | Predicts 14-day MACE in NSTEMI/UA. Guides invasive vs conservative strategy. | Score 0-2 = low risk. 3-4 = intermediate. 5-7 = high risk → early invasive strategy (cath within 24h). |
| TTE (echocardiogram) | Assess EF, regional wall motion abnormalities (correlate with ischemic territory), valvular disease. | New RWMA supports ACS. EF ≤ 40% → ACEI/ARB + aldosterone antagonist post-MI. Assess for mechanical complications. |
| CBC | Baseline Hgb for bleeding risk, platelets for DAPT safety. | Anemia may contribute to demand ischemia (Type 2 MI). Thrombocytopenia limits antiplatelet options. |
| BMP | Cr for contrast and medication dosing, K⁺/Mg²⁺ for arrhythmia risk. | Adjust heparin dosing for renal function. K⁺ > 4.0, Mg²⁺ > 2.0. |
| Coags, lipid panel | Baseline coags before anticoagulation. Lipid panel within 24h (LDL drops after 24-48h in acute MI). | Start high-intensity statin (atorvastatin 80 mg) regardless of LDL. |
| Class | Drug / Dose | Key Pearls |
|---|---|---|
| Aspirin | ASA 325 mg loading (chew), then 81 mg daily indefinitely | Give immediately on presentation. Non-enteric coated for faster absorption. Continue lifelong. |
| P2Y12 inhibitor | Ticagrelor (Brilinta) 180 mg load → 90 mg BID PREFERRED Clopidogrel (Plavix) 600 mg load → 75 mg daily Prasugrel (Effient) 60 mg load → 10 mg daily (post-PCI only) | Ticagrelor superior to clopidogrel PLATO, 2009. Prasugrel contraindicated if prior stroke/TIA, age ≥ 75, or weight < 60 kg. DAPT duration: minimum 12 months post-PCI. |
| Anticoagulation | Heparin (UFH) 60 U/kg bolus (max 4000 U) → 12 U/kg/hr (max 1000 U/hr) OR Enoxaparin 1 mg/kg SC q12h | Continue until cath or for duration of hospitalization if conservative strategy. Check aPTT q6h for UFH (goal 60-80s). Reduce enoxaparin to 1 mg/kg daily if CrCl < 30. |
| Beta-blocker | Metoprolol tartrate 12.5-25 mg PO q6-12h → titrate to HR 60-70 | Start within 24h if no HF, cardiogenic shock, bradycardia, or heart block. Avoid IV beta-blocker acutely (increased cardiogenic shock risk). Convert to succinate for discharge. |
| Statin | Atorvastatin (Lipitor) 80 mg daily PREFERRED OR Rosuvastatin 40 mg daily | High-intensity statin for ALL ACS regardless of baseline LDL. Start in-hospital. Do not check LDL to decide -just start it. |
| ACEi / ARB | Lisinopril 2.5-5 mg daily (start low) OR Losartan 25-50 mg daily if ACEi intolerant | Indicated if EF ≤ 40%, anterior MI, diabetes, or HTN. Start within 24h if hemodynamically stable (SBP ≥ 90). Continue indefinitely. |
| Nitroglycerin | NTG 0.4 mg SL q5min × 3 PRN chest pain NTG drip 5-200 mcg/min for refractory pain | Contraindicated if SBP < 90, RV infarct, PDE5 inhibitor within 24-48h. Provides symptom relief -does NOT reduce mortality. |
🧪 Workup: Focused labs + imaging → see Workup tab
⚡ Treat: Evidence-based algorithm → see Management tab
💊 Drugs: Key medications with dosing → see Medications tab
📣 Present: One-liner + key points → see Rounds tab
- Troponin rise + fall with ≥ 1 value > 99th percentile
- Ischemic symptoms or ECG changes (ST depression, TWI)
- UA = same presentation but troponin negative
- GRACE score determines invasive vs conservative strategy
- ASA 325 + P2Y12 load + heparin drip
- GRACE > 140 → cath within 24h (early invasive)
- Low GRACE → conservative: medical therapy + stress test
- Atorvastatin 80 mg, BB if no contraindication
- Dynamic ST changes
- Recurrent angina despite medical therapy
- Hemodynamic instability
- Elevated troponin trending up
- EF < 40% on echo
- Diabetes, CKD, prior PCI/CABG
- Switching heparin types (increases bleeding)
- Missing Wellens or de Winter pattern
- Not risk-stratifying with GRACE
- Discharging without follow-up plan
Arrhythmias
| Width | Regularity | Likely Rhythm | First-Line Treatment |
|---|---|---|---|
| Narrow (< 120 ms) | Regular | AVNRT (~60%), AVRT (~30%), atrial tachycardia (~10%) | Vagal maneuvers → adenosine 6 mg → 12 mg → 12 mg |
| Narrow | Irregular | Afib, Aflutter with variable block, MAT | See Afib topic. MAT → treat underlying (COPD, hypoxia, Mg/K). |
| Wide (> 120 ms) | Regular | VT until proven otherwise. Also: SVT with aberrancy, pre-excited tachycardia. | Treat as VT. Stable → amiodarone. Unstable → cardioversion. Pulseless → defibrillate. |
| Wide | Irregular | Afib with WPW (DANGEROUS), polymorphic VT / Torsades, Afib with aberrancy | Afib + WPW → procainamide or cardiovert. NEVER adenosine/CCB/BB. Torsades → Mg 2g IV + defibrillate if pulseless. |
▶ AVNRT vs AVRT, How to Identify (tap to expand)
- Slow pathway: slow conduction velocity, but SHORT refractory period (recovers quickly after firing).
- Fast pathway: fast conduction velocity, but LONG refractory period (slow to recover).
- A premature atrial contraction (PAC) fires earlier than the next expected sinus beat.
- The fast pathway is still in its long refractory period from the prior beat, so the PAC is blocked there.
- The slow pathway has already recovered (short refractory period), so the PAC travels DOWN the slow pathway.
- By the time the impulse reaches the distal AV node, the fast pathway has now recovered.
- The impulse turns around and travels retrograde UP the fast pathway back to the top of the AV node.
- At the top, the slow pathway has re-recovered, so the impulse descends it again.
- Steps 3 through 6 repeat continuously. The loop lives entirely inside the AV node and spins at ~150–220 bpm.
- Who: young to middle-aged adults, women > men, structurally normal hearts. Triggered by caffeine, alcohol, stress, stimulants.
- ECG during SVT: narrow QRS, regular, rate 150–220.
- P wave: buried in QRS or pseudo-R' in V1 (as described above).
- RP interval: very short (< 70 ms), classic "short RP" tachycardia.
- Baseline ECG (sinus rhythm): usually normal. No delta wave.
- No physiologic AV delay. It conducts as fast as ordinary atrial or ventricular muscle, so impulses cross it nearly instantly.
- Longer refractory period than the AV node (in most cases).
- May conduct in both directions, or only retrograde (ventricle to atrium), which is called a "concealed" pathway because the baseline ECG looks totally normal.
- Short PR interval (< 120 ms): the AV node delay is partially bypassed.
- Delta wave: a slurred, slow upstroke at the start of the QRS, caused by that early pre-excited myocardium depolarizing slowly from cell to cell before the His-Purkinje system catches up.
- Slightly widened QRS: a fusion beat of accessory-pathway conduction + normal node conduction.
- A PAC fires earlier than the next sinus beat.
- The accessory pathway is still refractory (longer refractory period than the AV node), so the PAC cannot cross it.
- The PAC travels down the AV node only. Ventricle depolarizes normally through His-Purkinje, producing a narrow QRS.
- By the time the ventricle is fully depolarized, the accessory pathway has now recovered.
- The impulse crosses retrograde UP the accessory pathway from ventricle back to atrium.
- The atrium is re-activated, and the impulse descends the AV node again.
- Steps 3 through 6 repeat at ~150–220 bpm. The circuit uses the WHOLE heart as its substrate: atrium, AV node, ventricle, accessory pathway, back to atrium.
- Who: often younger patients. Some have a known pre-excitation pattern (delta wave + short PR) on baseline ECG; others first present with SVT and have a concealed pathway.
- ECG during SVT: narrow QRS in orthodromic (~95%), wide QRS in antidromic (~5%).
- P wave: visible after the QRS, inverted in II/III/aVF (as described above).
- RP interval: long (> 70 ms).
- Baseline ECG (sinus rhythm): delta wave + short PR + slightly widened QRS if manifest WPW; completely normal if the pathway is concealed (retrograde-only).
| Feature | AVNRT | AVRT (Orthodromic) |
|---|---|---|
| Frequency | ~60% of PSVT | ~30% of PSVT |
| Circuit | Entirely within the AV node (dual pathways) | Uses an accessory pathway outside the AV node |
| P wave location | Buried in the QRS, OR pseudo-R' in V1 immediately after QRS | Visible after the QRS, on the ST segment or T wave (retrograde) |
| RP interval | Short (< 70 ms),"short RP" tachycardia | Long (> 70 ms), longer RP |
| Baseline ECG (sinus) | Normal | May show delta wave + short PR (manifest WPW); normal if pathway is concealed |
| QRS width during SVT | Narrow (unless pre-existing BBB) | Narrow in orthodromic (~95%); wide in antidromic (~5%) |
| Risk profile | Benign; recurrent episodes, not life-threatening | Accessory pathway + AFib → can conduct at 300+ bpm to ventricles → VF and sudden death |
| First-line acute treatment | Vagal maneuvers → adenosine 6 mg → 12 mg → 12 mg | Same for narrow/regular presentation. If AFib with pre-excitation: procainamide or cardioversion. NEVER adenosine / CCB / BB / digoxin. |
| Definitive therapy | Slow-pathway ablation (> 95% cure) | Accessory-pathway ablation (> 95% cure) |
- Narrow QRS, regular, rate 150–220? → PSVT (AVNRT or AVRT most likely).
- Look for the P wave:
- Buried in QRS or pseudo-R' in V1 → AVNRT.
- Visible after QRS, inverted in II/III/aVF → AVRT (orthodromic).
- Check a prior baseline ECG. Delta wave + short PR at rest → accessory pathway → AVRT.
- Adenosine response. Both terminate with adenosine (the AV node is part of both circuits), so response does NOT differentiate them during SVT. Adenosine is useful as a diagnostic tool when it transiently unmasks underlying atrial flutter or tachycardia.
| Feature | Favors VT | Favors SVT with Aberrancy |
|---|---|---|
| AV dissociation | ✅ Most specific for VT. P waves march independently at a different rate from QRS. | ❌ Absent -P waves are associated with each QRS (1:1 relationship). |
| Fusion & capture beats | ✅ Pathognomonic for VT. Fusion = P wave partially captures ventricle mid-VT. Capture = sinus beat "captures" ventricle (narrow QRS in midst of wide complexes). | ❌ Not seen. |
| QRS width | ✅ > 160 ms strongly favors VT. Extremely wide (> 200 ms) = almost certainly VT. | Typically 120–140 ms (bundle branch block pattern). |
| QRS morphology | ✅ Bizarre, atypical -doesn't look like a classic RBBB or LBBB pattern. | Looks like a typical RBBB or LBBB (rsR' in V1, or rS in V1 with broad R in V6). |
| Concordance | ✅ All precordial leads (V1–V6) deflect in the same direction (all positive or all negative) = VT. | ❌ Mixed precordial directions (typical R-wave progression). |
| Northwest axis | ✅ Extreme axis deviation (negative in I and aVF) = almost always VT. | Axis is within normal or expected BBB range. |
| RS interval in precordial leads | ✅ RS interval > 100 ms in any precordial lead (Brugada criterion) favors VT. | RS interval < 100 ms. |
| Absence of RS complex | ✅ No RS complex in any V1–V6 lead (all QS or monophasic R) = VT. | RS complexes present in at least one precordial lead. |
| History | ✅ Prior MI, known cardiomyopathy, HF, structural heart disease -VT is overwhelmingly more likely. | Young, no structural heart disease, known SVT/BBB on prior ECG. |
| Hemodynamic stability | ⚠️ Does NOT help differentiate. VT can be hemodynamically stable. Do not assume stable = SVT. | ⚠️ Same -SVT with aberrancy can also be unstable. |
| Response to adenosine | ❌ No effect (VT does not involve AV node). ⚠️ Adenosine is generally safe but NOT diagnostic -VT that doesn't terminate ≠ SVT. | ✅ Terminates or slows (involves AV node reentry). But only give if you're reasonably confident it's SVT. |
Step 1: Absence of RS complex in ALL precordial leads? → VT
Step 2: RS interval > 100 ms in any precordial lead? → VT
Step 3: AV dissociation present? → VT
Step 4: Morphology criteria for VT in V1 and V6? → VT
If none of the above → SVT with aberrancy. Sensitivity > 98% for VT.
- Sawtooth pattern in II, III, aVF (best seen in II). Rate typically ~300 bpm with 2:1 block → ventricular rate ~150 bpm.
- If the ventricular rate is exactly ~150 bpm → think flutter until proven otherwise.
- Management: same as Afib (rate control, anticoagulation by CHA₂DS₂-VASc). Often responds better to cardioversion and ablation than to drugs.
- Ablation cure rate for typical (CTI-dependent) flutter is > 95% -refer early.
- ≥ 3 distinct P-wave morphologies with varying P-P, PR, and R-R intervals. Irregular rhythm.
- NOT Afib -MAT has discrete P waves before each QRS (Afib has no organized P waves).
- Almost always associated with severe underlying illness: COPD exacerbation, hypoxia, hypercapnia, hypomagnesemia, heart failure, theophylline use.
- Treatment = treat the underlying cause. Correct Mg²⁺ and K⁺. Improve oxygenation. Treat COPD.
- ⚠️ Do NOT cardiovert MAT -it will not work (multiple foci, not a single reentrant circuit).
- If rate control needed: IV magnesium 2g first. Then non-dihydropyridine CCB (verapamil/diltiazem) if no HF. Avoid beta-blockers in COPD-driven MAT.
- Junctional escape rhythm (40–60 bpm): narrow QRS, absent/retrograde P waves. Occurs when SA node fails or slows (sinus bradycardia, sick sinus, high vagal tone).
- Accelerated junctional rhythm (60–100 bpm): enhanced automaticity of AV junction. Causes: digoxin toxicity (#1), inferior MI, post-cardiac surgery, myocarditis.
- Junctional tachycardia (> 100 bpm): rare in adults. Think dig toxicity or post-surgical.
- Treatment: identify and treat the cause. If dig toxicity → hold digoxin, check level, give Digibind if hemodynamically unstable.
| Type | Cause | Key Features |
|---|---|---|
| Acquired (most common) | Drugs (see table below), electrolyte abnormalities (hypoK, hypoMg, hypoCa), bradycardia, hypothermia, structural heart disease | Reversible -stop offending agent, correct electrolytes |
| Congenital -LQT1 | KCNQ1 mutation (K⁺ channel) | Events triggered by exercise (especially swimming). Beta-blockers effective. |
| Congenital -LQT2 | KCNH2 (hERG) mutation (K⁺ channel) | Events triggered by auditory stimuli (alarm clock, phone). Beta-blockers + avoid triggers. |
| Congenital -LQT3 | SCN5A mutation (Na⁺ channel) | Events at rest/sleep. Beta-blockers less effective. May need ICD + mexiletine. |
| Category | Drugs |
|---|---|
| Antiarrhythmics | Amiodarone, sotalol, dofetilide, procainamide, quinidine, ibutilide |
| Antibiotics | Fluoroquinolones (levofloxacin, moxifloxacin), macrolides (azithromycin, erythromycin), TMP-SMX |
| Antifungals | Fluconazole, voriconazole |
| Antipsychotics | Haloperidol, quetiapine, ziprasidone, chlorpromazine |
| Antiemetics | Ondansetron (IV doses > 16 mg), droperidol |
| Antidepressants | Citalopram, escitalopram (dose-dependent), TCAs |
| Other | Methadone, hydroxychloroquine, sumatriptan |
- ECG pattern: Coved ST elevation (> 2 mm) with T-wave inversion in V1–V3 (Type 1 = diagnostic). Type 2 (saddleback) is suggestive but not diagnostic. Consider high V1–V2 leads (2nd/3rd intercostal space) to unmask.
- Risk: Sudden cardiac death from VF, often during rest or sleep. Young males (20–40), Southeast Asian descent.
- Genetics: SCN5A mutation (Na⁺ channel loss-of-function) in ~20–30% of cases. Autosomal dominant.
- Triggers (avoid): Fever (#1, aggressive antipyretics for any febrile illness), sodium channel blockers (Class I antiarrhythmics, TCAs, cocaine, propofol in high doses), electrolyte disturbances, alcohol, large meals at night.
- Provocation test: IV procainamide, ajmaline, or flecainide, unmasks Type 1 pattern in ambiguous cases. Do only in controlled EP lab setting.
- Management: ICD if prior cardiac arrest, spontaneous Type 1 pattern with syncope, or sustained VT. Quinidine (unique sodium-channel blocker that paradoxically helps in Brugada, blocks Ito current). Isoproterenol drip for electrical storm. Family screening with ECG.
- Do NOT give Class I antiarrhythmics (flecainide, procainamide, lidocaine, except for provocation testing), they worsen the ECG and increase VF risk.
- ECG triad: Short PR (< 120 ms) + delta wave (slurred QRS upstroke) + wide QRS (> 120 ms). Caused by an accessory pathway (Bundle of Kent) bypassing the AV node.
- Orthodromic AVRT (~95%): Impulse goes DOWN the AV node, UP the accessory pathway. Narrow QRS. Treat like SVT (adenosine safe).
- Antidromic AVRT (~5%): Impulse goes DOWN the accessory pathway, UP the AV node. Wide QRS -looks like VT. Procainamide or cardiovert.
NEVER give AV nodal blockers: adenosine, beta-blockers, calcium channel blockers, digoxin. These block the AV node and force ALL conduction down the accessory pathway.
Treatment: Procainamide IV (slows accessory pathway) or synchronized cardioversion. If unstable → immediate cardioversion.
| Feature | PAC (Premature Atrial Contraction) | PVC (Premature Ventricular Contraction) |
|---|---|---|
| Origin | Ectopic atrial focus (above AV node) | Ventricular myocardium (below AV node) |
| P Wave | Present -early, abnormal morphology (differs from sinus P) | Absent -no preceding P wave |
| QRS | Narrow (< 120 ms) -conducts normally through His-Purkinje | Wide & bizarre (> 120 ms) -cell-to-cell spread, NOT His-Purkinje |
| QRS Axis | Same as baseline -normal conduction pathway preserved | Different from baseline -axis points away from PVC origin. RVOT PVCs → LBBB + inferior axis. LV PVCs → RBBB morphology. |
| Compensatory Pause | Usually non-compensatory (incomplete) -SA node resets | Usually full compensatory pause -SA node not reset |
| Pulse on Exam | Normal pulse -patient may feel a brief "skip" | Weaker pulse (↓ filling time → ↓ stroke volume). May drop the beat entirely on radial pulse. Followed by a stronger "thud" beat after the pause. |
| Clinical Significance | Almost always benign. Common with caffeine, stress, alcohol. Frequent PACs may predict future Afib. | Benign if: < 10% burden, structurally normal heart, asymptomatic. ⚠️ Concern if: > 10–15% burden (PVC-induced cardiomyopathy), R-on-T phenomenon, post-MI. |
| Aberrancy Clue | Very early PACs may conduct aberrantly (usually RBBB pattern -right bundle has longer refractory period) → wide QRS but axis still normal | Always wide QRS with abnormal axis. If wide-complex beat has same axis as baseline → think aberrant PAC, not PVC. |
| Management | Reassurance. Reduce caffeine/alcohol if symptomatic. Rarely need treatment. | < 10% burden + normal echo: reassure, BB if symptomatic. > 10–15% burden: echo to check EF, consider ablation. CAST, 1991 -⚠️ do NOT suppress PVCs with Class Ic agents post-MI. |
- Definition: SA node dysfunction causing alternating bradycardia (sinus bradycardia, sinus pauses, sinoatrial exit block) and tachycardia (paroxysmal Afib, atrial flutter, atrial tachycardia).
- Presentation: Syncope, presyncope, fatigue, exercise intolerance. Often elderly with fibrosis of the SA node.
- Diagnostic clue: Bradycardia that doesn't respond to atropine + intermittent tachyarrhythmias.
- Treatment: Permanent pacemaker (allows safe use of rate-control drugs for the tachycardia component). Without a pacer, rate-controlling drugs worsen the bradycardia.
- Key point: You can't treat the tachy without a pacer to protect against the brady.
| Parameter | Frequency | Target |
|---|---|---|
| Continuous telemetry | Until rhythm stable ×24h | Identify recurrence, assess rate control |
| 12-lead ECG | After conversion + daily | Confirm sinus rhythm, rule out pre-excitation (delta wave → WPW) |
| Vitals | q4h | HR, BP -especially after starting rate/rhythm control agents |
| Electrolytes | Daily | K⁺ > 4.0, Mg²⁺ > 2.0 (low levels promote arrhythmia) |
| Presentation | Treatment |
|---|---|
| Pulseless VT | Defibrillate (unsynchronized) 120–200J biphasic. Start CPR. Follow ACLS arrest protocol. |
| Unstable VT with pulse | Synchronized cardioversion 100–200J. Sedate first if time permits. |
| Stable monomorphic VT | Amiodarone 150 mg IV over 10 min → 1 mg/min × 6h → 0.5 mg/min × 18h. Alternative: procainamide 20–50 mg/min until rhythm converts (monitor QRS width and BP). Lidocaine 1–1.5 mg/kg as third option. |
| Polymorphic VT / Torsades | Magnesium 2g IV push. If pulseless → defibrillate (unsynchronized). Stop QT-prolonging drugs. Overdrive pacing or isoproterenol to increase HR (shortens QT). IV potassium to K⁺ > 4.5. |
- Step 1: Treat the underlying cause -optimize COPD, correct hypoxia, treat HF/sepsis.
- Step 2: IV magnesium 2g -often converts or slows MAT.
- Step 3: If rate control needed → non-dihydropyridine CCB (verapamil/diltiazem). Avoid beta-blockers if COPD is the driver.
- ⚠️ Cardioversion does NOT work for MAT -multiple automatic foci, not a reentrant circuit.
- ⚠️ Antiarrhythmics are not effective -focus on the underlying disease.
| Rhythm | Synchronized? | Energy (Biphasic) | Notes |
|---|---|---|---|
| SVT | ✅ Synchronized | 50–100J | Sedate first (propofol, midazolam, or etomidate) |
| Atrial Flutter | ✅ Synchronized | 50–100J | Often converts at low energy |
| Atrial Fibrillation | ✅ Synchronized | 120–200J | Higher energy needed. Anticoagulate ≥ 3 weeks pre or TEE to rule out LAA thrombus. |
| Monomorphic VT (stable) | ✅ Synchronized | 100J → 200J → 300J → 360J | Escalate if first shock fails |
| Polymorphic VT / Torsades | ❌ Unsynchronized (DEFIB) | 120–200J | Can't sync to irregular rhythm -treat as VF |
| VF / Pulseless VT | ❌ Unsynchronized (DEFIB) | 120–200J | ACLS protocol. CPR between shocks. |
Vitals: HR 182 (regular), BP 108/72, RR 18, SpO₂ 99% on RA.
ECG: Narrow-complex regular tachycardia at 180 bpm. No discernible P waves. No delta wave on prior baseline ECG.
Question: What is the most likely rhythm and your first intervention?
Management: Most likely AVNRT (most common SVT in young women). Start with modified Valsalva per REVERT, 2015 (blow into syringe 15s → lie flat with legs raised 15s). If unsuccessful, Adenosine (Adenocard) 6 mg rapid IV push → 12 mg if no response. Post-conversion ECG confirms sinus rhythm with no pre-excitation. Discharge with cardiology referral for EP study and catheter ablation (cure rate >95%).
Vitals: HR 146 (irregularly irregular with pauses), BP 98/64, RR 20, SpO₂ 94% on 2L NC.
ECG: Atrial tachycardia with variable block. Multiple P-wave morphologies with grouped beating pattern. Baseline ST scooping ("digitalis effect").
Question: Is this MAT or digitalis toxicity? What is your next step?
Management: Classic digitalis toxicity, atrial tachycardia with block + GI symptoms + visual changes. Hold digoxin immediately. Check digoxin level (therapeutic 0.5–2.0 ng/mL), K⁺ (hypokalemia worsens toxicity), Mg²⁺, and Cr. Distinguish from MAT (≥3 P-wave morphologies, seen in severe COPD). If hemodynamically unstable or level markedly elevated, give Digoxin Immune Fab (Digibind). Replete K⁺ >4.0 and Mg²⁺ >2.0. Avoid cardioversion (risk of refractory VF in dig toxicity).
Vitals: HR 224 (irregular), BP 82/50, RR 24, SpO₂ 92% on RA.
ECG: Wide-complex irregular tachycardia. Varying QRS morphology. Rates 180–260 bpm. Consistent with pre-excited atrial fibrillation (Afib conducting over the accessory pathway).
Question: What drugs must you avoid and why?
Management: Avoid ALL AV nodal blockers, Adenosine (Adenocard), Diltiazem (Cardizem), Metoprolol (Lopressor), and Digoxin (Lanoxin) are contraindicated. These slow AV node conduction but leave the accessory pathway uninhibited → unopposed rapid conduction → ventricular fibrillation. Given hemodynamic instability, proceed to synchronized cardioversion (120–200J biphasic). If stable, use Procainamide (Pronestyl) 15–17 mg/kg IV to slow accessory pathway conduction. Urgent cardiology consult for catheter ablation.
| Parameter | Frequency | Target / Action |
|---|---|---|
| CRP | Weekly until normal | Guides duration of therapy. Do NOT taper NSAIDs until CRP normalizes. Premature taper = recurrence. |
| ECG | At diagnosis, then at follow-up | Monitor ST/PR normalization through 4 stages. Persistent changes may suggest constrictive physiology. |
| TTE (Echo) | Repeat in 1-2 weeks | Confirm effusion resolution. Repeat sooner if hemodynamic compromise or clinical worsening. |
| Symptoms | Each visit | Pleuritic chest pain, dyspnea, positional symptoms. Worsening = consider effusion enlargement or recurrence. |
| Renal function (Cr) | 1-2 weeks after starting NSAIDs | NSAID nephrotoxicity. Check BMP especially in elderly, CKD, heart failure, or concurrent ACEi/ARB. |
| Activity restriction | Until CRP normal + asymptomatic | Non-athletes: restrict until symptom resolution. Athletes: no competitive sports for minimum 3 months (6 months if myopericarditis). |
| Parameter | Frequency | Target |
|---|---|---|
| Continuous telemetry | Until rhythm stable ×24h | Identify recurrence, assess rate control |
| 12-lead ECG | After conversion + daily | Confirm sinus rhythm, rule out pre-excitation (delta wave → WPW) |
| Vitals | q4h | HR, BP -especially after starting rate/rhythm control agents |
| Electrolytes | Daily | K⁺ > 4.0, Mg²⁺ > 2.0 (low levels promote arrhythmia) |
- 12-lead ECG during tachycardia -narrow complex (< 120 ms)? Regular or irregular? P waves visible? Relationship of P to QRS? Short RP vs long RP? These features differentiate AVNRT, AVRT, and atrial tachycardia.
- Adenosine (6 mg → 12 mg rapid IV push) -diagnostic AND therapeutic. Terminates re-entrant SVTs involving the AV node (AVNRT, AVRT). If it doesn't terminate but reveals underlying atrial activity (flutter waves, atrial tachycardia) → the diagnosis is NOT AVNRT/AVRT.
- BMP -K⁺ (hypokalemia triggers arrhythmias), Mg²⁺ (low Mg → refractory hypoK and arrhythmias), Ca²⁺ (hypercalcemia can shorten QT)
- TSH -hyperthyroidism is a common reversible cause of SVT and atrial fibrillation. Check in all new-onset SVT.
- Troponin -if prolonged SVT (sustained rapid rates can cause demand ischemia, especially in CAD patients) or if chest pain is present
- Echocardiogram -if recurrent SVT, to assess for structural heart disease (WPW with accessory pathway, hypertrophic cardiomyopathy, valvular disease). Not urgent for first isolated episode with normal ECG.
| Class | MOA | Drugs | Clinical Use | ⚠️ Side Effects |
|---|---|---|---|---|
| Ia Na⁺ channel block (intermediate) | Blocks Na⁺ channels + K⁺ channels → slows conduction + prolongs repolarization. Widens QRS and prolongs QT. | Procainamide (Pronestyl) Quinidine Disopyramide (Norpace) | VT, SVT, Afib, WPW (procainamide). Brugada VF storm (quinidine). | ⚠️ Procainamide: drug-induced lupus (chronic use), QT prolongation → Torsades, agranulocytosis ⚠️ Quinidine: cinchonism (tinnitus, HA, vision changes), diarrhea, thrombocytopenia, QT prolongation |
| Ib Na⁺ channel block (fast) | Blocks Na⁺ channels with fast kinetics → shortens repolarization. Works preferentially on ischemic/depolarized tissue. | Lidocaine (Xylocaine) Mexiletine (Mexitil) | VT/VF (acute, especially ischemia-related). Mexiletine for congenital LQT3. Lidocaine for refractory VF in ACLS. | ⚠️ Lidocaine: CNS toxicity (seizures, confusion, perioral numbness, tremor), bradycardia ⚠️ Mexiletine: GI upset, tremor, dizziness |
| Ic Na⁺ channel block (slow) | Potent Na⁺ channel blockade with slow kinetics → markedly slows conduction. Minimal effect on repolarization. | Flecainide (Tambocor) Propafenone (Rythmol) | Afib/flutter (rhythm control) -"pill-in-pocket" for paroxysmal Afib. SVT. Only in structurally normal hearts. | ⚠️ CAST trial: increased mortality 3.6× post-MI CAST, 1991 ⚠️ Contraindicated in structural heart disease, CAD, HF ⚠️ Proarrhythmic (can organize Afib → flutter with 1:1 conduction → always co-prescribe AV nodal blocker) |
| II Beta-blockers | Block β₁-adrenergic receptors → decrease SA node automaticity, slow AV conduction, reduce myocardial O₂ demand. | Metoprolol (Lopressor) Esmolol (Brevibloc) (ultra-short acting) Atenolol (Tenormin) Propranolol (Inderal) | Rate control (Afib, SVT, sinus tachycardia). Suppress PVCs. Congenital long QT (LQT1, LQT2). Post-MI arrhythmia prevention. | ⚠️ Bradycardia, hypotension, bronchospasm (non-selective), fatigue, depression, mask hypoglycemia in diabetics ⚠️ Do NOT stop abruptly -rebound tachycardia/hypertension |
| III K⁺ channel blockers | Block K⁺ channels → prolong repolarization (action potential duration) → prolong QT interval. | Amiodarone (Cordarone) Sotalol (Betapace) Dofetilide (Tikosyn) Ibutilide (Corvert) | Amiodarone: VT, VF, Afib, almost any arrhythmia (Swiss army knife). Sotalol: Afib, VT. Dofetilide: Afib maintenance. Ibutilide: acute Afib/flutter conversion. | ⚠️ Amiodarone (multiple organ toxicity): pulmonary fibrosis, thyroid dysfunction (hypo & hyper -contains iodine), hepatotoxicity, corneal microdeposits, peripheral neuropathy, blue-gray skin, photosensitivity, QT prolongation ⚠️ Sotalol: QT prolongation → Torsades, bradycardia (also has Class II activity) ⚠️ Dofetilide: must be initiated inpatient (3-day telemetry) -QT prolongation risk. Renally dosed. ⚠️ Ibutilide: QT prolongation → Torsades (monitor 4–6h post-infusion) |
| IV Ca²⁺ channel blockers (non-DHP) | Block L-type Ca²⁺ channels in SA/AV node → slow AV conduction and decrease heart rate. | Diltiazem (Cardizem) Verapamil (Calan) | Rate control (Afib, SVT). Acute SVT termination. AVNRT/AVRT (second-line after adenosine). | ⚠️ Hypotension, bradycardia, constipation (verapamil), peripheral edema ⚠️ NEVER in WPW + Afib (enhances accessory pathway conduction → VF) ⚠️ NEVER in decompensated HF (negative inotropy worsens failure) ⚠️ Avoid with beta-blockers IV (additive AV block risk) |
| Drug | MOA | Clinical Use | ⚠️ Side Effects |
|---|---|---|---|
| Adenosine (Adenocard) | Activates A₁ adenosine receptors → transient AV node block (6-second half-life) | First-line for stable narrow-complex SVT (AVNRT/AVRT). Diagnostic (unmasks underlying rhythm). 6 mg → 12 mg → 12 mg rapid IV push. | ⚠️ Transient: chest tightness, flushing, dyspnea, sense of doom (warn patient!) ⚠️ Contraindicated in WPW + Afib, severe asthma, 2nd/3rd degree heart block ⚠️ Theophylline/caffeine antagonize. Dipyridamole/carbamazepine potentiate → reduce dose. |
| Digoxin (Lanoxin) | Inhibits Na⁺/K⁺-ATPase → increases vagal tone (slows AV conduction). Also increases intracellular Ca²⁺ → positive inotropy. | Rate control in Afib (especially with HF -provides inotropy + rate control). Third-line in most settings. | ⚠️ Narrow therapeutic window (0.5–2.0 ng/mL). Toxicity: N/V, visual changes (yellow halos), arrhythmias (accelerated junctional, bidirectional VT, PAT with block) ⚠️ Hypokalemia and hypomagnesemia worsen toxicity ⚠️ Toxicity antidote: Digibind (digoxin-specific Fab antibodies) |
| Magnesium | Stabilizes cardiac cell membranes. Suppresses early afterdepolarizations. Essential cofactor for Na⁺/K⁺-ATPase. | First-line for Torsades de Pointes. Adjunct in MAT. Electrolyte repletion in any arrhythmia. | ⚠️ Flushing, hypotension (if given too fast), loss of deep tendon reflexes (toxicity), respiratory depression (severe toxicity) |
| Atropine | Muscarinic (M₂) receptor antagonist → blocks vagal input to SA/AV node → increases HR and conduction. | First-line for symptomatic bradycardia. 0.5 mg IV q3–5min (max 3 mg). Bridge to transcutaneous/transvenous pacing. | ⚠️ Tachycardia, urinary retention, dry mouth, mydriasis, delirium (especially elderly) ⚠️ Ineffective in infranodal block (Mobitz II, 3rd degree with wide escape) -go straight to pacing |
🧪 Workup: 12-lead ECG, BMP (K⁺, Mg²⁺), TSH, trop if chest pain
⚡ Treat: Vagal → adenosine → cardioversion if unstable
💊 Maintenance: Metoprolol, diltiazem, or flecainide/sotalol for recurrent
📈 Monitor: Telemetry, ECG post-conversion, electrolytes
📣 Present: See Rounds tab
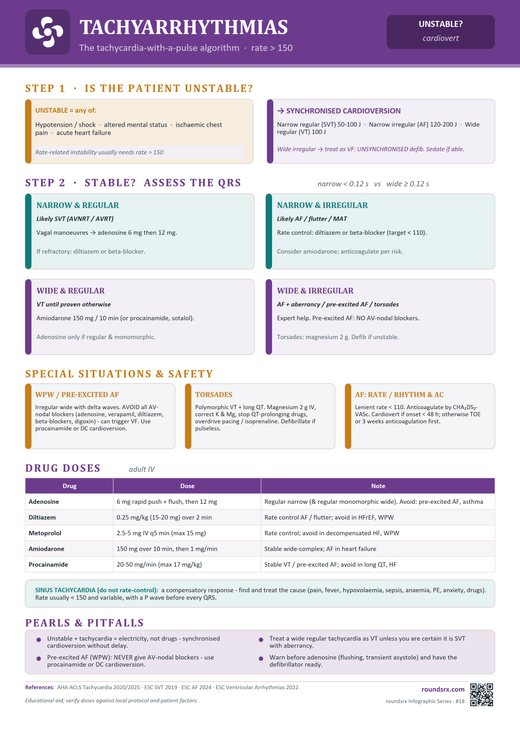 ⤢ Tap to open full size
⤢ Tap to open full size
Text version
- AV nodal blockers in WPW → VF
- Not trying modified Valsalva first
- Missing atrial flutter (2:1 looks like SVT at 150)
- Adenosine in wide-complex tachycardia